Valvular Problems
There are four heart valves: two atrioventricular valves (mitral and tricuspid) and two semilunar valves (aortic and pulmonic). It is the coordination of the opening and closing of these valves with the pressure gradients created during the phases of the cardiac cycle that determines the forward flow of the blood. During systole, the aortic and pulmonic valves are normally open, and the mitral and tricuspid valves are closed. During diastole, the mitral and tricuspid valves are open, and the aortic and pulmonic valves are closed.
Valvular disease causes disruption of normal blood flow through the valves, damaging the valves and impeding cardiac function to various degrees. The types of valvular disease are defined according to the valve affected and the type of functional alteration or stenosis due to a narrowed orifice and regurgitation due to incomplete closure. Although any of the valves may be affected, those on the left side of the heart are more commonly affected. Valvular problems may be congenital or acquired. At one time, most acquired valvular disease in the United States was a result of rheumatic fever, but other causes are more common today, such as atherosclerotic heart disease in the elderly.
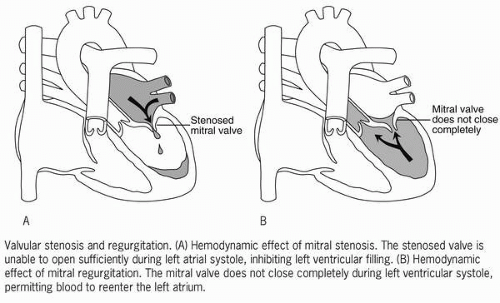 |
Mitral valve stenosis is a valve in which the leaflets have become thickened and restrict the forward flow of blood, thereby increasing the workload of the chamber behind the diseased valve. As a result, left atrial pressure increases to compensate for the resistance to outflow (increased afterload) and the chamber hypertrophies.
 The types of valvular disease are defined according to the valve affected and the type of functional alteration or stenosis due to a narrowed orifice and regurgitation due to incomplete closure.
The types of valvular disease are defined according to the valve affected and the type of functional alteration or stenosis due to a narrowed orifice and regurgitation due to incomplete closure.Mitral valve regurgitation (also called incompetence or insufficiency) occurs when an incompetent valve does not close completely, permitting backward or retrograde flow of blood during ventricular systole into the chamber above the valve. This causes an increased volume of blood, which increases workload and causes hypertrophy of the affected chamber. The mitral and aortic valves are more commonly affected than the tricuspid and pulmonic valves.
The dilation and hypertrophy that occur are compensatory mechanisms to support the pumping ability of the heart. Eventually, contractility and the ejection fraction may diminish, the end-diastolic pressure increases, and the ventricles fail. Abnormal valves also predispose to cardiac infection and thrombus formation. Cardiac dysrhythmias, particularly atrial fibrillation, artial flutter, and atrioventricular blocks, may occur.
 Abnormal valves also predispose to cardiac infection and thrombus formation.
Abnormal valves also predispose to cardiac infection and thrombus formation.Mitral valve prolapse syndrome is the most common valve disorder in the United States and is more prevalent in young women. It is also associated with other inherited connective tissue disorders. Mitral valve prolapse syndrome is caused by the displacement of the posterior cusp of the mitral valve, causing the valve leaflets to bulge or balloon upward into the left atrium during systole. It has a high incidence, suggesting that it may be a normal variant rather than pathological. It is usually associated with minimal morbidity or mortality, and, although rare, severe sequelae are potentially possible such as mitral regurgitation, ventricular failure, thromboemboli, and sudden death.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


