Urinary Diversion Surgery
A urinary diversion provides an alternative route for urine excretion when pathology impedes normal flow through the bladder. Most commonly performed in patients who have undergone a cystectomy, diversion surgery also may be performed in patients with a congenital urinary tract defect; a severe, unmanageable urinary tract infection (UTI) that threatens renal function; chronic cystitis, an injury to the ureters, bladder, or urethra; an obstructive malignancy; or a neurogenic bladder.
There are several ways that urinary diversion surgery can be performed. Possible procedures include ileal conduit (also known as ureteroileal urinary conduit, ileal bladder, ileal loop, Bricker’s operation, and ureteroileostomy), continent internal ileal reservoir (also known as a Kock pouch), and orthotopic bladder replacement. (See Common types of urinary diversion, pages 930 and 931.
Urinary diversions may be categorized as incontinent or continent. Incontinent diversions include the ileal conduit, ureterosigmoidostomy, and nephrostomy. With these types, urine flow is constant and an external collection device is required permanently. Continent diversions include the Kock pouch, Indiana pouch, Mainze reservoir, and Camey procedure (also known as the orthotopic bladder replacement). The advantage of these procedures is that an external collection bag isn’t needed. However, not all patients are candidates for continent diversion surgery, and there is the possibility of urine leakage after the creation of a continent diversion.
Ileal conduit, the most common urinary diversion, involves anastomosis of the ureters to a small portion of the ileum excised especially for the procedure, followed by the creation of a stoma from one end of the ileal segment. This resulting stoma is called a urostomy. It drains urine continuously and requires the patient to wear an external pouch at all times.
A ureterosigmoidostomy is an internal urinary diversion that redirects urine through the colon and then out the rectum. Because this detour into the colon causes two major complications—metabolic disorders (hyperchloremic acidosis) and pyelonephritis—it isn’t frequently performed. To be a candidate for this procedure, the patient must have a competent internal sphincter because urine excretion will occur from the rectum permanently. The drainage from the rectum will have the consistency of watery diarrhea, which can result in acidosis and electrolyte imbalances involving potassium, chloride, and magnesium. Pyelonephritis occurs as a result of reflux of bacteria from the colon.
Continent internal ileal reservoir, such as the Kock pouch or Indiana pouch, is another type of urinary diversion. Following cystectomy, a segment of the small bowel or colon is used to create an internal pouch. For the Kock pouch, the ureters are then implanted into the sides of the pouch, with each ureter intussuscepted to create a nipple valve. The efferent ureter and nipple valve are brought to the skin surface of the anterior abdomen as a stoma and prevent leakage of urine from the pouch. The afferent ureter and nipple valve prevent urine reflux.
Ureters are implanted differently in the Indiana pouch. They are tunneled through the tenia of the segment of colon used to construct the pouch.
Because the pouch on these two procedures is internal and can be trained to hold urine without leakage, it allows the patient to remain free from external appliances. It does, however, require the patient to catheterize the abdominal opening intermittently so as to empty the pouch.
The continent internal ileal reservoir has recently been modified so that the reservoir has both the ureters and urethra connected to it. This eliminates the need for a small opening in the abdominal wall and helps preserve the patient’s body image. However, unless the lower portion of the bladder can be spared, continence depends solely on the urethra and external sphincter. Consequently, total bladder
substitution is usually limited to males because their longer urethra permits better external sphincter control. Drainage ofthe internal pouch relies on passive emptying when the external sphincter is relaxed and on abdominal straining. If these techniques aren’t sufficient, the patient must learn to do intermittent self-catheterization. Complications, such as tumor recurrence in the urethra and frequent nocturnal enuresis, can affect up to 50% of patients and are major drawbacks of the procedure.
substitution is usually limited to males because their longer urethra permits better external sphincter control. Drainage ofthe internal pouch relies on passive emptying when the external sphincter is relaxed and on abdominal straining. If these techniques aren’t sufficient, the patient must learn to do intermittent self-catheterization. Complications, such as tumor recurrence in the urethra and frequent nocturnal enuresis, can affect up to 50% of patients and are major drawbacks of the procedure.
Another possible procedure is a nephrostomy, which is a short-term technique that diverts urine away from an obstruction or lesion below the level of the renal pelvis.
Common types of urinary diversion
Types of urinary diversion include ileal conduit, orthotopic bladder replacement, and continent internal ileal reservoir (Kock pouch).
Ileal conduit
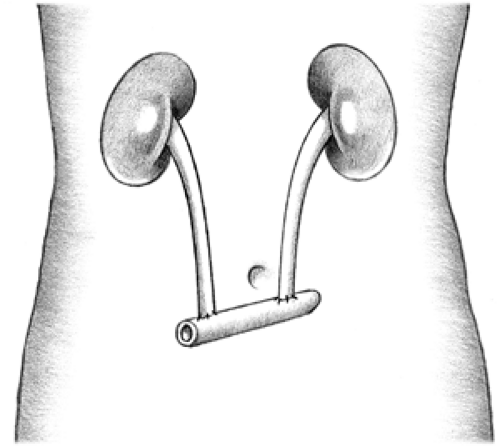 Figure. No caption available |
Both ureters are anastomosed to a small segment of ileum, one end of which is brought to the surface of the lower abdomen to form a stoma.
Orthotopic bladder replacement
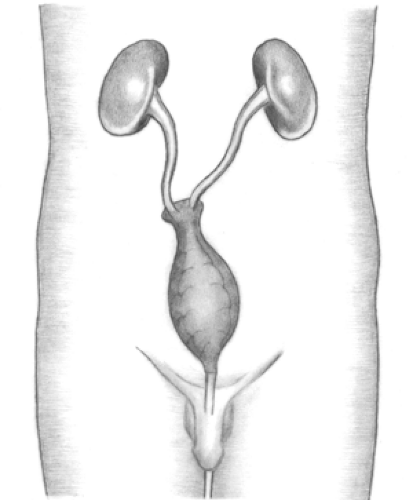 Figure. No caption available |
An internal pouch is created from the small bowel or small and large bowel. The urethral stump is anastomosed to the pouch. The patient voids through the urethra. This procedure is performed in males only. The patient commonly experiences nocturnal incontinence.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Get Clinical Tree app for offline access
