Trauma to the Nervous System
Any trauma to the head (skull, scalp, or brain) increases the risk of damage to the underlying structures and the potential for permanent damage or death. Some initial injuries are very apparent, while the extent of other injuries may not be obvious for several days after the incident.
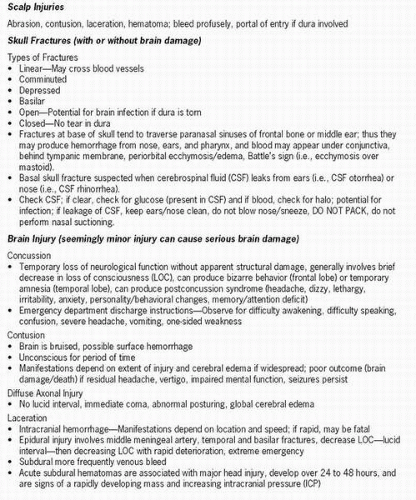 Figure 16-1 Types of head injury. |
 Figure 16-1 Continued |
Head injury includes injury to the scalp, skull, or brain. The major risk in head injury is damage to the brain from bleeding, swelling, and increasing intracranial pressure (ICP), with the potential for disability or death.
Two million head injuries occur each year in the United States, and approximately 75,000 to 100,000 patients die of the injury. Seventy thousand to 90,000 injuries are severe enough to cause permanent brain dysfunction. Most deaths are immediate from direct trauma, massive hemorrhage, and shock. Deaths may occur within a few hours from progressive bleeding or within weeks from multisystem failure.
The major causes of head injury are due to motor vehicle accidents (50%), falls (21%), assaults (12%), and sports injuries (10%). Firearmsrelated head injuries are increasing. Two-thirds of head injuries are in individuals younger than 30 years old, with males outnumbering females 3:1. The second highest incidence is among the elderly.
The incidence of head injuries has been reduced due to recent safety guidelines and public awareness of the importance of wearing helmets during sports, installation of air bags in automobiles, and use of passive seat restraints.
Pathophysiology
The brain is protected from external injuries by hair, skin, and the skull. Damage to the brain occurs as a result of compression of the skull from impact, which compromises integrity of the bone. The amount of damage depends on the force of the injury.
 Head injuries are divided into two categories: primary or direct injuries (damage is caused by the impact) and secondary injuries that result in brain swelling, infection, and hypoxia of the cerebral tissue.
Head injuries are divided into two categories: primary or direct injuries (damage is caused by the impact) and secondary injuries that result in brain swelling, infection, and hypoxia of the cerebral tissue.Head injuries are divided into two categories: primary or direct injuries (damage is caused by the impact) and secondary injuries that result in brain swelling, infection, and hypoxia of the cerebral tissue. Head injuries are also referred to as closed or blunt trauma and open or penetrating trauma.
Mechanisms of trauma include deformation, acceleration-deceleration as seen in coup-countercoup injury, and diffuse axonal injury. The injuries may be insignificant or may lead to poor outcomes. Factors predictive of poor outcomes include intracranial hematoma, increasing age, abnormal motor signs, impaired or absent eye movements or pupil reflexes, early sustained hypotension, hypoxemia/hypercapnia, and ICP > 20 mm Hg. Scalp injuries such as abrasions, contusions, lacerations, and hematomas often bleed profusely, but most are benign and only significant if associated with meningeal tears.
Skull fractures occur with or without brain injury. The major complications of skull fractures are intracranial infections, bleeding and hematomas, meningeal tears, brain tissue damage, and increased ICP. The location of a fracture may be significant, as a basilar fracture generally crosses the paranasal sinuses in the frontal bone or the middle ear in the temporal bone, causing meningeal tears that result in cerebrospinal
fluid (CSF) fistulas, increasing the risk of infection. In addition, blood may collect around the eyes or ears.
fluid (CSF) fistulas, increasing the risk of infection. In addition, blood may collect around the eyes or ears.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


