|

Define the terms nursing process and holistic caring process.
Outline the steps of the holistic caring process.
Explore the ways in which conceptual models of nursing inform and guide the holistic caring process.
Discuss the ways in which standards of holistic nursing practice are incorporated into the holistic caring process.
Analyze the assessment tool that you are using in clinical practice to determine whether the tool is consistent with a holistic nursing perspective.
Explore the ways to document holistic nursing care in a computerized electronic health record (EHR) through use of standardized terms such as those found in nursing diagnostic taxonomies, the Nursing Interventions Classification, and the Nursing Outcomes Classification.
Identify the nursing concerns and activities most relevant to your clients.
Integrate prevention, health promotion, and wellness diagnoses into practice.
Use the Trifocal Model as an organizing structure for a visual composite of the three levels of a person’s health patterns in prioritizing and planning nursing interventions and patient outcomes within the nurse-person interaction.
Implement the Holistic Nursing: Scope and Standards of Practice (2007) of the American Holistic Nurses Association (AHNA) and American Nurses Association (ANA) in your work and life.
Observe the pattern appraisal and identification process in your everyday life as you walk into a new situation.
Identify the four patterns of knowing (empirical, ethical, aesthetic, and personal knowledge) as they guide you within the nurse-person interaction.
Develop and trust your intuitive thinking processes when assessing clients’ conditions.
Evaluate the impact of intuitive thinking in both your professional and personal lives.
Explore your own beliefs and values regarding the concepts of holistic nursing.
Write down specific examples of holistic nursing care while reflecting on your enactment of the holistic caring process.
Assessment
Diagnosis, or identification of problems or needs, or pattern recognition
Plan of care
Implementation or intervention
Evaluation
creating a calming atmosphere), nutrition (timing of meals and presentation of food and fluids), sleep (relaxation, back rubs), or skin integrity (massage, turning, and attention to bed linens) were carried out by nurses but often referred to as “common sense” rather than as professional responses to identified client needs. The concept of a nursing process allowed nurses to use a common language, systematize nursing practice and education, and enhance nursing autonomy.
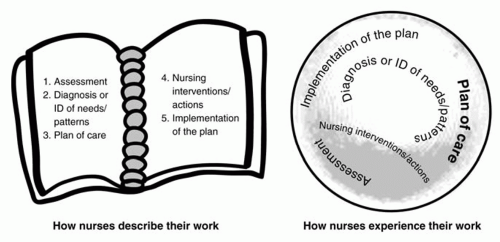 FIGURE 7-1 Two Conceptualizations of the Nursing Process Source: © Noreen C. Frisch, 2007. |
science and objectivity as the only source of knowing. Further, some believe that the nursing process serves the interests of the profession over the interests of the clients and are concerned with use of labels and jargon. The nursing process is atheoretical and is compatible with a variety of philosophical positions. The problem may not lie in the nursing process per se, but rather in the differing philosophic perspectives used to describe it.
| |||||||||||||||||||||||||||||||||||||||
concept of emotional intelligence suggests that emotional intelligence facilitates interpretation of the nurse’s perceptions.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


