During seclusion, a patient is separated from others in a safe, secure, and contained environment with close nursing supervision to protect himself, other patients, and staff members from imminent harm. Seclusion is used when nonphysical interventions are ineffective. Follow your facility’s policy when placing a patient in seclusion, and familiarize yourself with the Joint Commission’s standards on the use of seclusion for behavioral health care reasons in nonbehavioral health care settings.
Seclusion is based on three principles: containment, isolation, and decreased sensory input. In containment, the patient is restricted to an area in which he can be protected from harm. Moreover, others are protected from impulsive acts by the patient. Isolation permits the patient to withdraw from situations that are too intense for him to handle at that point. Decreased sensory input reduces external stimulation and sensory overload, allowing the patient to regroup and reorganize coping skills.
ESSENTIAL DOCUMENTATION
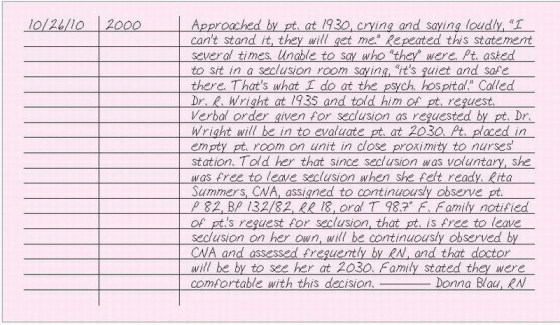
Record the date and time of each episode as well as the rationale for, and circumstances leading up to, the use of seclusion. Describe the nonphysical interventions that were tried first. In your note, chart the time that you notified the family members and their names. Document that you notified the doctor and obtained a verbal or written order. Enter the verbal order in the doctor’s orders, according to your facility’s policy. Record each time the order for seclusion is renewed. Record the doctor’s visit and his evaluation of the patient. Criteria for ending seclusion should be charted. Document what the patient was told about seclusion, including the behavior criteria for stopping seclusion. Chart your frequent assessments of the patient, such as nutrition, hydration, circulation, range of motion, mobility, hygiene, elimination, comfort, and psychological status. Record your interventions to help the patient meet these needs. Describe your interventions to help the patient reduce his need for seclusion and his responses to these interventions. Document that the patient is receiving continuous monitoring while in seclusion and by whom.
SEIZURE MANAGEMENT
Seizures are paroxysmal events associated with abnormal electrical discharges of neurons in the brain. Partial seizures are usually unilateral, involving a localized or focal area of the brain. Generalized seizures involve the entire brain.
When your patient has a generalized seizure, observe the seizure characteristics to help determine the area of the brain involved; administer anticonvulsants as ordered; protect him from injury; and prevent serious complications, such as aspiration and airway obstruction. When caring for a patient at risk for seizures, take precautions to prevent injury and complications in the event of a seizure.
PREVENTING SEIZURES
Teach the patient the following measures to help him control and decrease the occurrence of seizures:
Take the exact dose of medication at the times prescribed. Missing doses, doubling doses, or taking extra doses can cause a seizure.
Eat balanced, regular meals. Low blood glucose levels (hypoglycemia) and inadequate vitamin intake can lead to seizures.
Be alert for odors that may trigger an attack.Advise the patient and his family to inform the doctor of any strong odors they notice at the time of a seizure.
Limit alcohol intake.The patient should check with the doctor to find out whether he can drink alcoholic beverages at all.
Get enough sleep. Excessive fatigue can precipitate a seizure.
Treat a fever early during an illness. If the patient can’t reduce a fever, he should notify the doctor.
Learn to control stress. If appropriate, suggest learning relaxation techniques such as deep-breathing exercises.
Avoid trigger factors, such as flashing lights, hyperventilation, loud noises, heavy musical beats, video games, and television.
ESSENTIAL DOCUMENTATION
If a patient is at risk for seizures, document all precautions taken, such as padding the side rails, headboard, and footboard of the bed; keeping the bed in low position; raising side rails while the patient is in bed; and having suction equipment nearby. Record that seizure precautions have been explained to the patient.
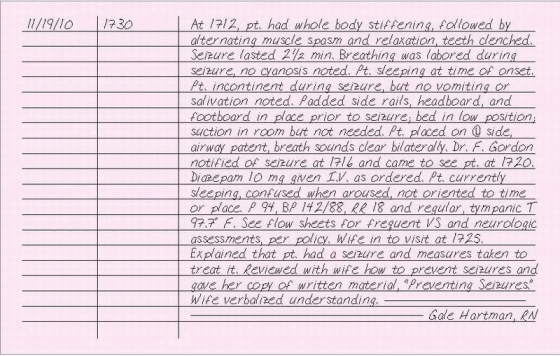
If your patient has a seizure, record the date and time it began as well as its duration and any precipitating factors. Identify any sensation that may be considered an aura. Describe involuntary behavior occurring at the onset, such as lip smacking, chewing movements, or hand and eye movements. Record any incontinence, vomiting, or salivation during the seizure. Describe where the movement began and the parts of the body involved. Note any progression or pattern to the activity. Document whether the patient’s eyes deviated to one side and whether the pupils changed in size, shape, equality, or reaction to light. Note if the patient’s teeth were clenched or open.
Document the patient’s response to the seizure, drugs given, complications, and interventions. Record the name of the doctor that you notified, the time of notification, and any orders given. Finally, record your assessment of the patient’s postictal mental and physical status every 15 minutes for 1 hour, every 30 minutes for 1 hour, and then hourly as long as there are no further complications, or according to your facility’s policy.
Document patient teaching that you provide for the patient or his family, including instructions you give about preventing and managing seizures. (See Preventing seizures)
SEXUAL ADVANCE BY COLLEAGUE
The Equal Employment Opportunity Commission defines sexual harassment as an unwelcome sexual advance, a request for sexual favors, and other verbal, nonverbal, or physical conduct of a sexual nature. However, such behavior as sexual activity between consenting adults or asking someone for a date isn’t sexual harassment. Sexual harassment is a subtle but real form of sexual abuse. (See Myths about sexual harassment,page 366.)
An unwanted sexual advance by a colleague should be addressed immediately. Decline the advance in a direct and honest manner. However, if your colleague persists, or if the initial advance consists of sexually charged, degrading, or vulgar words or makes you a target of sexual jokes, touching, or pinching, tell the colleague making the advance that this behavior is harassment and that it won’t be tolerated.
MYTHS ABOUT SEXUAL HARASSMENT
Common myths about sexual harassment include:
If women would just say “No,” it would stop.
Harassment will stop if a person just ignores it.
If women watched the way they dress, there wouldn’t be a problem with sexual harassment.
Only women can be sexually harassed.
Sexual harassment is no big deal — it’s the natural way men and women express affection and friendship.
Most people enjoy sexual attention at work.Teasing and flirting make work fun.
Sexual harassment is harmless. Persons who object have no sense of humor or don’t know how to accept a compliment.
Sexual harassment policies will negatively affect friendly relationships.
Nice people couldn’t possibly be harassers.
Most facilities have a policy for filing a complaint. If your facility doesn’t have a policy, inform your immediate supervisor or the human resources department that the behavior you experienced constitutes sexual harassment, and ask how to proceed with a complaint.
The human resources department will contact the accused employee and inform him that a complaint has been filed against him. They’ll advise the employee that this behavior must cease immediately. After you’ve reported the harassment, it’s the responsibility of your employer to follow through according to local and federal guidelines. Confidentiality is important, and the privacy of individuals reporting or accused of sexual harassment must be protected as much as possible. A complaint may also be filed with the state Human Rights Commission or with the federal Equal Employment Opportunity Commission.
ESSENTIAL DOCUMENTATION
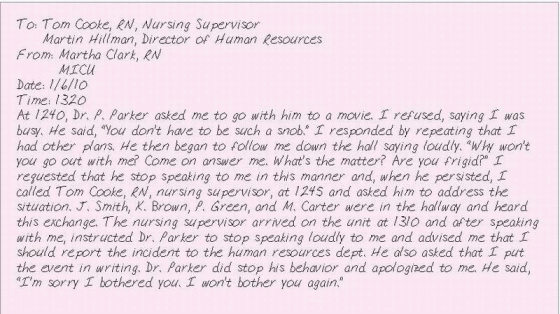
States vary in the way that sexual harassment issues are addressed and resolved. The human resources department in your facility can help you with documentation that complies with local and federal law and facility policy. In general, documentation should include:
description of the incident, including the date, time, and location
statements made by both parties (in quotes)
names of individuals that you informed about the incident, such as the nursing supervisor and human resources manager, and their responses
date, time, and location where the information was shared as well as any counseling or referral offered to you
names of witnesses, if any
names of anyone who supports your charge (other victims or witnesses).
Document each instance of harassment. Keep a copy of all the documentation at home. This will be useful if legal action is taken.
SEXUAL ADVANCE BY PATIENT
Several recent studies show that more than 50% of nurses have experienced sexual harassment on the job and more than 25% reported being victimized while on the job. Patients were the most frequent sources of sexual harassment and physical assault. Nursing, by its very nature of having to care for a patient’s bodily needs, transgresses normal social rules regarding physical contact. A patient who relies on a nurse’s caring attitude may exploit this. In addition, the intimacy of the nurse-patient relationship can mislead a patient into believing that a nurse might be receptive to such an advance.
The patient’s motivation for making a sexual advance may be a need for friendliness or attention, a demonstration of anger, or a plea for reassurance about sexual attractiveness. In many cases, when a sexual advance by a patient occurs, the nurse will typically ignore it, pretend she hasn’t heard it, or withdraw from contact with the patient. However, a better way to handle this type of behavior is to address it immediately and to be honest and direct with the patient, making a comment such as “I’m uncomfortable when you speak to me like that. Let’s talk about something else” or “I don’t want you to touch me that way.”
If a verbal warning isn’t effective in changing the patient’s behavior, inform your nursing supervisor immediately and have a colleague present when care is delivered. In addition, speak with the patient’s doctor about the patient’s behavior. Consultation with psychiatric staff may help the patient control inappropriate behavior. Also, the psychiatric clinical nurse specialist can help the nursing staff plan this patient’s care. Be sure to maintain the patient’s privacy and confidentiality, discussing his behavior only with caregivers who need to know.
ESSENTIAL DOCUMENTATION
Follow your facility’s policy for documenting a sexual advance by a patient. In addition to documenting the incident in the medical record, you may be required to fill out an incident report.
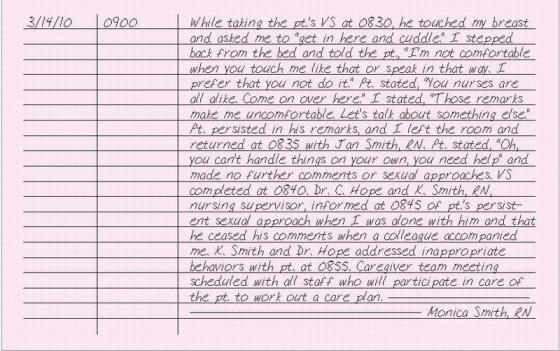
Record the date and time that the sexual behavior took place. Carefully document the care that the patient received as well as the inappropriate behavior. Record what the patient said to you, using his words (in quotes). List staff members who witnessed the behavior. Leave your emotions or feelings out of your charting. Document your response to the patient’s behavior, putting your exact statements in quotes. Record the time that you notified the doctor and nursing supervisor, their names, and their responses.
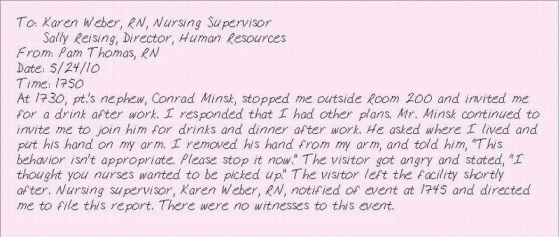
SEXUAL ADVANCE BY VISITOR
The Equal Employment Opportunity Commission defines sexual harassment as unwelcome sexual advances, requests for sexual favors, and other verbal, nonverbal, or physical conduct of a sexual nature. Unwelcome sexual advances may come from anyone, including a person visiting a patient.
Address an unwanted sexual advance by a family member or visitor immediately. Tell the family member or visitor to stop the behavior; that it’s inappropriate and won’t be tolerated. If you don’t feel comfortable confronting the family member or visitor, your facility should have a policy in place designating who will address this behavior. Your employer is responsible for ensuring that you’re supported and protected from reprisals.
Immediately report the incident to the nursing supervisor and the human resources department. Most facilities have a policy for filing a complaint. If a policy doesn’t exist, ask the nursing supervisor or human resources department how to proceed with a complaint.
ESSENTIAL DOCUMENTATION
Document sexual advances by a family member or visitor according to your facility’s policy. Record the date, time, and location of the incident as well as the name of the family member or visitor. Describe the person’s behaviors and record what was said, using his words (in quotes). Document the names of any witnesses, and note whether sexual advances were made to other staff members. Record the name of the nursing supervisor and the time of notification. Write a separate report for each instance of harassment.
SHOCK
Shock is a systemic pathologic event characterized by diffuse cellular ischemia that can lead to cell, tissue, and organ death if not promptly recognized and treated. Shock is classified as hypovolemic, cardiogenic, or distributive. Distributive type is further divided into septic, neurogenic, and anaphylactic shock. (See Classifying shock.)
Because shock either causes or results from multisystem failure, it’s typically treated in an intensive care unit. Nursing responsibilities related to shock center on prevention, early detection, emergent treatment, and support during recovery and rehabilitation.
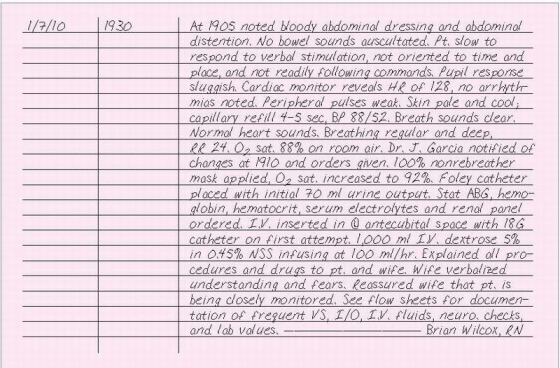
ESSENTIAL DOCUMENTATION
Record the date and time of your entry. Document your assessment findings of shock, such as declining level of consciousness, hypotension, tachycardia in early shock and bradycardia in later shock, ECG changes, weakened pulses, dyspnea, tachypnea, declining arterial oxygen saturation and partial pressure of arterial oxygen, rising partial pressure of arterial carbon dioxide, respiratory and metabolic acidosis, oliguria, rising blood urea nitrogen and creatinine, diminished or absent bowel sounds, and pale, cool skin. Note the time that you notified the doctor, his name, and orders given, such as drug, fluid, blood, and oxygen administration. Record your interventions, such as assisting with the insertion of hemodynamic monitoring lines, inserting I.V. lines, administering drugs, continuous ECG monitoring, providing supplemental oxygen, inserting an indwelling urinary catheter, airway management, and pulse oximetry monitoring. Chart your patient’s responses to these interventions. Use flow sheets to record your frequent assessments, vital signs, hemodynamic measurements, intake and output, I.V. therapy, and laboratory test and arterial blood gas values. Also, record patient and family teaching and emotional care given.
CLASSIFYING SHOCK
Type
Description
Hypovolemic
Results from a decrease in central vascular volume.Total body fluids may or may not be decreased. Causes include hemorrhage, dehydration, and fluid shifts (trauma, burns, anaphylaxis).
Cardiogenic
Results from a direct or indirect pump failure with decreasing cardiac out put. Total body fluid isn’t decreased. Causes include valvular stenosis or insufficiency, myocardial infarction, cardiomyopathy, arrhythmias, cardiac arrest, cardiac tamponade, pericarditis, pulmonary hypertension, and pulmonary emboli.
Distributive
Results from inadequate vascular tone that leads to massive vasodilation. Vascular volume remains normal and heart pumps adequately, but size of vascular space increases, causing maldistribution of blood within the circulatory system. It includes the following subtypes:
▪ Septic shock—A form of severe sepsis characterized by hypotension and altered tissue perfusion.Vascular tone is lost and cardiac output may be decreased.
▪ Neurogenic shock—Characterized by massive vasodilation from loss or suppression of sympathetic tone. Causes include head trauma, spinal cord injuries, anesthesia, and stress.
▪ Anaphylactic shock—Characterized by massive vasodilation and increased capillary permeability secondary to a hypersensitivity reaction to an antigen.
SICKLE CELL CRISIS
Sickle cell anemia is a genetic disorder that occurs primarily, but not exclusively, in African Americans. It results from a defective hemoglobin molecule (hemoglobin S) that causes red blood cells to roughen and become sickle-shaped. Such cells impair circulation, resulting in chronic ill health (characterized by fatigue, dyspnea on exertion, and swollen joints), periodic crises, long-term complications, and premature death.
Although sickle cell anemia is a chronic disorder, acute exacerbations or crises periodically occur. If you suspect your patient with sickle cell anemia is in a crisis, notify the doctor immediately and anticipate oxygen and I.V. fluid administration and pain control.
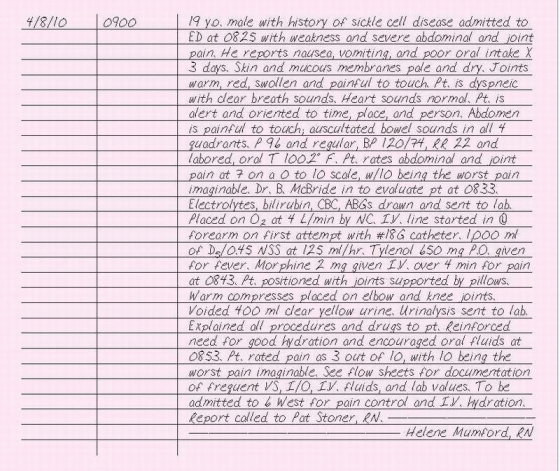
ESSENTIAL DOCUMENTATION
Record the date and time of your entry. Document your assessment findings of a sickle cell crisis, such as severe abdominal, thoracic, muscular, and joint pain; jaundice; fever; dyspnea; pallor; and lethargy. Note the time that you notified the doctor, his name, and orders given, such as oxygen administration, analgesics, antipyretics, fluid administration, and blood transfusions. Record your interventions, such as initiating I.V. therapy using a large-bore catheter for blood and fluid administration, encouraging bed rest, placing warm compresses over painful joints, and administering drugs and oxygen. Chart your patient’s responses to these interventions. Use flow sheets to record your frequent assessments as well as the patient’s vital signs, intake and output, I.V. therapy, and laboratory test values. Document any patient teaching performed (crisis prevention, genetic screening) and emotional support given.
SKIN CARE
In addition to helping shape a patient’s self-image, the skin performs many physiologic functions. It protects internal body structures from the environment and potential pathogens, regulates body temperature and homeostasis, and serves as an organ of sensation and excretion. As a result, meticulous skin care is essential to overall health.
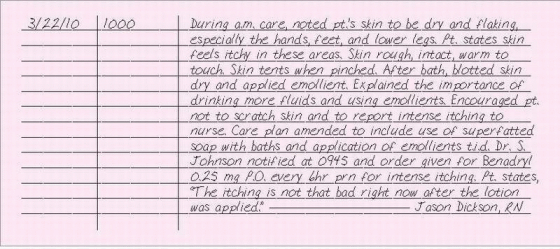
ESSENTIAL DOCUMENTATION
Record the date and time of your entry. Assess your patient’s skin and describe its condition, noting changes in color, temperature, texture, tone, turgor, thickness, moisture, and integrity. Describe your interventions related to skin care and the patient’s response. Note the time that you notified the doctor of any changes, his name, the orders given, your actions, and the patient’s response. Describe patient teaching given, such as proper hygiene and the importance of turning and positioning every 2 hours.
SKIN GRAFT CARE
A skin graft consists of healthy skin taken from either the patient (autograft) or a donor (allograft) that is then applied to a part of the patient’s body. The graft resurfaces an area damaged by burns, traumatic injury, or surgery. Care procedures for an autograft or allograft are essentially the same. However, an autograft requires care for two sites: the graft site and the donor site.
Successful grafting depends on various factors, including clean wound granulation with adequate vascularization, complete contact of the graft with the wound bed, aseptic technique to prevent infection, adequate graft immobilization, and skilled care. Depending on your facility’s policy, a doctor or specially trained nurse may change graft dressings.
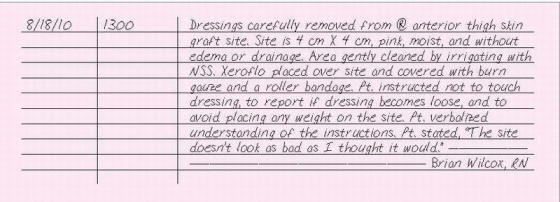
ESSENTIAL DOCUMENTATION
Record the date and time of each dressing change. Note the location, size, and appearance of the graft site. Document all drugs used, and note the patient’s response to these drugs. Describe the condition of the graft, and note any signs of infection or rejection. Chart the name of the doctor that you notified, the time of notification, and any concerns or complications discussed. Record the specific care given to the graft site, including how it was covered and dressed. Document any patient and family teaching that you provide and evidence of their understanding. Note the patient’s reaction to the graft.
SMOKING
It’s a well-known fact that smoking has adverse effects on health. Yet people continue to smoke—even in the hospital. Smoking in the hospital poses special risks beyond the usual health risks: secondhand smoke can aggravate many illnesses, fire and explosion may occur when a person smokes in an area where oxygen is being used, and a smoldering cigarette dropped in a wastebasket or on bed linens can start a fire.
Explain your facility’s smoking policy to the patient on admission, and provide him with a written set of facility rules, if available. If you find your patient smoking in a nonsmoking area, remind him of the facility’s smoking policy. Ask him to extinguish his smoking materials and to move to a designated smoking area, if possible. Alert the doctor if your patient is smoking against medical advice.
Only gold members can continue reading. Log In or Register to continue