Research, Evidence, Quality Improvement, Safety, Diversity, and Health Policy
Research, Evidence-Based Practice, and Clinical Decision Making
Tara Trimarchi
Research
Research as a Basis for Clinical Practice
Evidence from well-designed research studies results in better outcomes.
The U.S. Department of Health and Human Services Office of Extramural Research and the National Institute of Health define research as “a systematic investigation designed to develop new knowledge.”
The National Institute of Nursing Research (NINR) is a branch of the National Institute of Health. The NINR states that the purposes of nursing research is to develop the knowledge to:
Build the scientific foundation for clinical practice.
Prevent disease and disability.
Manage and eliminate symptoms caused by illness.
Enhance end-of-life and palliative care.
The process of knowledge creation and translation includes concept development, from basic scientific discovery through clinical trials, and dissemination of the research findings.
As described in Figure 24.1, the process of clinical research can be integrated with the process of patient care.
The highest priority of clinical research is to protect human subjects from undue harm and burden from participation in the study.
Special oversight for studies is often required when the research subjects are children. For the purpose of research, the National Institutes of Health defines a child as an individual who is under 21 years of age.
A health care organization’s institutional review board (IRB) reviews research protocols for appropriateness and safety, and approves research proposals before studies can be conducted (NINR, 2008).
Steps to Conducting Clinical Research
Identification of the research question.
Systematic review of literature related to the phenomenon in question.
Formation of the hypothesis.
Design of the study.
Approval to perform study from the IRB.
Conduct of the study—consenting subjects, administration of study interventions, monitoring, and data collection.
Analysis of the data and interpretation of the findings.
Summary of the study, its findings, and conclusions prepared as a manuscript for publication.
Roles of Care Providers in Clinical Research
Intervention design and implementation planning within the clinical setting.
Participant recruitment and consenting.
Maintenance of human subjects’ protection standards.
Participant education and support.
Direct administration of study interventions and evaluations.
Participant monitoring for response and adverse events.
Data preparation and management.
Dissemination of research findings.
Research Involving Children
Andrea M. Kline-Tilford
Definitions in Research
Children
Individuals who have not yet attained the legal age for consent of treatments/procedures in the proposed research.
Parent
Child’s biologic or adoptive parent.
Guardian
An individual authorized to consent on the behalf of a child to general medical care under state or local law.
 FIGURE 24.1 • Clinical Research. From Hastings, C. E., Fisher, C. A., & McCabe, M. A. (2012). Clinical research nursing: A critical resource in the national research enterprise. Nursing Outlook, 60(3), 149-156. |
Ward
A child whose welfare is determined by the state, institution, or entity.
Categories of Research Involving Children
Research not involving greater-than-minimal risk:
Appropriate provisions are needed for obtaining and documenting the assent from the child.
Appropriate provisions are in place for obtaining the permission of at least one of the child’s parents.
Research involving greater-than-minimal risk with the prospect of direct benefit to individual study participants as long as the following issues are addressed:
The risk of the study is justified by the anticipated benefit to the study participants.
The anticipated benefit to study participation is at least as favorable to the study participants as the benefits of alternative available approaches/therapies.
Appropriate provisions are made to obtain and document the assent of children and the permission of at least one of the child’s parents.
Research involving greater-than-minimal risk and no prospect of direct benefit to individual study participants, but likely to yield generalizable knowledge about the study participants’ disorder or condition as long as the following issues are addressed:
Anticipated risk represents only a minor increase over minimal risk.
Study intervention or procedure presents experiences that are reasonably commensurate with those encountered in the study participants’ actual or expected medical therapy.
Study intervention or procedure is likely to yield generalizable knowledge about the study participants’ disorder or condition, which is of vital importance for the understanding of the condition.
Appropriate provisions are made to obtain and document the assent of children and the permission of at least one of the child’s parents.
Special circumstances in pediatric research:
The requirement for permission of study participation may be waived in conditions when asking for parent/guardian permission is not reasonable (e.g., child maltreatment), and an appropriate mechanism to provide study participant protection is substituted.
Children who are wards of the state or other agency may be included in study participation if the study is related to their status as wards or is conducted in settings (e.g., schools, camps, hospitals) when the majority of study participants are not wards.
A child advocate must be appointed in these cases.
Ethical Concepts
Beneficence—doing for the good or welfare of the patient, research participant.
Maleficence—doing or causing harm.
Nonmaleficence—first, do no harm.
Malevolence—having or showing a desire to cause harm to another person.
Principle of double effect—performing an action that potentially causes a good effect, but also has a bad effect.
Consent and Assent
Shannon Konierczki
First statement on informed consent, parental permission, and assent was initially drafted and presented to the American Academy of Pediatrics Committee of Bioethics in 1985.
The issue of informed consent and permission, especially as it pertains to pediatric patients, continues to be an important topic of discussion and practice.
Consent is the act of decision making for oneself, so it is not a term that is commonly applied to the pediatric patient, but to their parent or guardian.
Informed consent is based on the cultural and legal assumption that a person of the age of majority has the full and accurate information needed to make a decision.
The decision-maker is traditionally assumed to have the mental capacity and ability to recognize the probable consequences of the decision.
In order to obtain informed consent for a pediatric patient, the parent must be provided with sufficient information to understand and authorize the recommended treatment.
Health care providers seeking consent should provide parents with information on the nature of the condition, the nature of the proposed diagnostic steps or treatment, and the probability of success. The parent should also be informed of the risks and benefits that may be involved, as well as the consequence of no treatment and alternative treatment options. The health care providers should then assess the parents’ understanding of the presented information by asking them questions or by asking them to explain the information.
In some cases, informed consent can be waived, such as in medical emergencies, public health emergencies, or when parents cannot be reached.
Assent is the ethical duty to inform and educate the pediatric patient in an age-appropriate way of an upcoming treatment or procedure, and to allow the child to participate in the decision making about the proposed care.
To acknowledge the child’s emerging capacities, honor their point of view, and promote well-being, health care providers should seek the child’s assent when possible.
In addition to parental permission.
Although children cannot be treated as rational, autonomous decision-makers, health care providers should give serious consideration to the patient’s developing capacities for participating in decision making.
Involving the child in discussions about their health care fosters trust and allows for a better patient-health care provider relationship.
Four elements of assent should be recognized:
Help the patient to achieve developmentally appropriate awareness of his or her condition.
Explain to the child what he or she can expect from the test and treatment.
Make a clinical assessment of the patient’s understanding of the situation, and determine whether the patient is being inappropriately pressured.
Determine whether the patient is willing to accept the proposed care.
Asking for assent facilitates involvement in care, which offers a way to gain control and respect as the child transitions from dependent to independent.
Care of the Emancipated Minor
Jessica L. Diver
An emancipated minor is one who has been granted autonomy from their parent or legal guardian.
This declaration allows minor patients the ability to make their own health care decisions prior to the age that is typically considered adulthood.
Events leading to emancipation may include pregnancy or marriage.
Emancipation may also be achieved by petition to the court in order to obtain financial control or gain independence, or for complete removal from a negative home life, among other indications.
Requirements for emancipation vary, as do the state laws regulating this status.
Due to the lack of federal laws or consensus regarding emancipated minors, each state establishes its own criteria.
While caring for emancipated minors, the health care provider should ensure confidentiality, communicate clearly and completely with the patient, and obtain consent from the minor.
Evidence-Based Practice
Tara Trimarchi
An approach to practicing health care that includes:
Awareness of the evidence to support clinical practices.
Ability to evaluate research to determine the strength of the evidence.
Use of strongest evidence to make clinical decisions.
The evidence-based practice (EBP) process includes (1) literature review; (2) critical appraisal of the quality of the research (see “levels of evidence” below); (3) application of the findings from the strongest studies to clinical practice; and (4) evaluation of the outcome of implementation of the EBPs.
Levels of evidence from strongest (1) to weakest (7) are:
Level 1: systematic review and meta-analysis of randomized controlled trials; clinical guidelines based on systematic reviews or meta-analyses.
Level 2: one or more randomized controlled trials.
Level 3: controlled trial (no randomization).
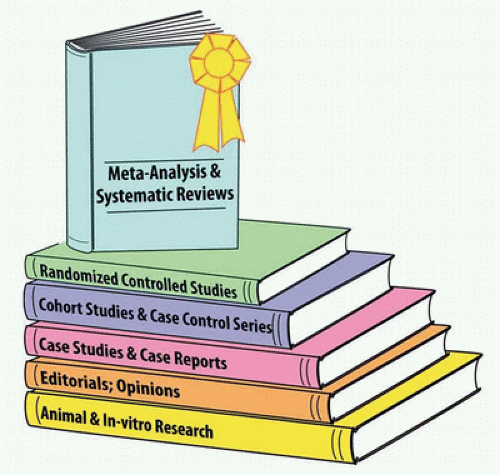
FIGURE 24.2 • Levels of Evidence Pyramid.
Level 4: case-control or cohort study.
Level 5: systematic review of descriptive and qualitative studies.
Level 6: single descriptive or qualitative study.
Level 7: expert opinion (Figure 24.2).
Clinical decision making.
Using EBP to guide clinical decision making requires performance of a literature search and review of studies for their relevance, strengths, and limitations.
The steps to conducting a literature search include:
Identify the clinical question(s).
Determine the most appropriate database to search for research that addresses the question.
Enter key words and phrases to find relevant literature— combine search terms as needed to find relevant literature.
Review the research studies for strength of the evidence.
Apply the strongest evidence in clinical practice.
EBP can be disseminated to clinicians for use in decision making via research committees, clinical census workgroups, and journal clubs.
EBPs can also be facilitated by clinical decision-support systems that are embedded into care delivery workflow, such as the inclusion of evidence-based care pathways and order sets in electronic health records and computerized provider order entry systems.
Quality Improvement and Patient Safety
Tara Trimarchi
Patient Safety
Background/Overview of Patient Safety
In 1999, the Institute of Medicine (IOM) report To Err Is Human: Building a Safer Health System documented that approximately 100,000 people died every year in the United States as the result of medical errors made by health care professionals.
Children are more likely than adults to experience medication errors or adverse drug events and experience a higher rate of diagnostic-related events, such as an incorrect diagnosis.
Definitions of Patient Safety Events
Adverse events are events in which injury to a patient is caused by medical management rather than by a patient’s underlying disease.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Get Clinical Tree app for offline access
