Renal Calculi and Benign Prostatic Hypertrophy
The presence of renal calculi (urolithiasis), which can range in size from microscopic to several centimeters in diameter, is the most common cause of renal system obstruction. Calculi are more common in men than in women, are more likely in whites than in African Americans, and develop most frequently between the ages of 20 and 40. The most common sites for stone formation are the renal pelvis, ureters, and bladder.
Although the prostate is part of the male reproductive system rather than the renal system, some diseases of the prostate can cause prostate enlargement, with effects on the renal and urinary systems.
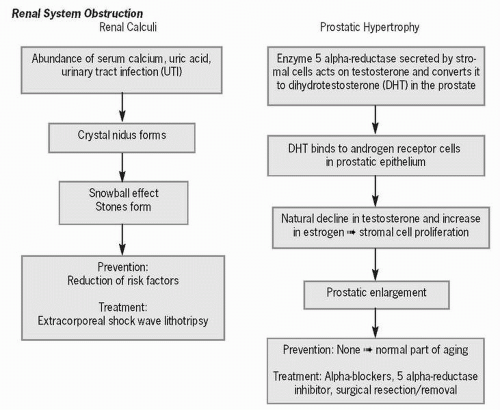 Figure 62-1 Renal system obstruction. |
Approximately 10% to 15% of individuals have renal calculi during their lifetime, with people living in the southern and midwestern United States at greatest risk for calculi development (thought to be related to high humidity levels and high temperature). Each year approximately 1 million people are hospitalized because of renal calculi and another 1 million are treated for this condition on an out patient basis.
 The presence of renal calculi is the most common cause of renal system obstruction.
The presence of renal calculi is the most common cause of renal system obstruction.It is estimated that over 50% of men over the age of 50 and 80% of men over the age of 70 will develop benign prostatic hyperplasia (BPH), a nonmalignant enlargement of the prostate gland and a significant
cause of urinary tract infection in men. This condition accounts for approximately 4 million office visits per year in the United States. The only identified risk factor thus far related to BPH is aging.
cause of urinary tract infection in men. This condition accounts for approximately 4 million office visits per year in the United States. The only identified risk factor thus far related to BPH is aging.
 The only identified risk factor thus far related to BPH is aging.
The only identified risk factor thus far related to BPH is aging.Pathophysiology
Renal calculi, polycrystalline aggregates of crystals, form either because of metabolic abnormalities, such as an urinary tract infection (UTI) or an aberrant urine pH. Normally, we are protected from calculi development by calculi inhibitors, including citrate, magnesium, and pyrophosphate, and endogenous compounds secreted by renal tubular cells, specifically nephrocalcin, uropontin, and Tamm-Horsfall protein.
When a nucleus (nidus) of crystals or organic material forms in the urinary tract and ions precipitate out of the urine and stick to the nucleus, a stone forms, much like a snowball that forms a larger and larger mass when rolled in the snow. Approximately 75% of renal calculi are calcium based, 10% are uric acid based, and 14% have a magnesium ammonium phosphate (i.e., struvite) base formed by urea-splitting bacteria associated with a UTI.
 Approximately 75% of renal calculi are calcium based, 10% are uric acid based, and 14% have a magnesium ammonium phosphate (i.e., struvite) base formed by urea-splitting bacteria associated with a UTI.
Approximately 75% of renal calculi are calcium based, 10% are uric acid based, and 14% have a magnesium ammonium phosphate (i.e., struvite) base formed by urea-splitting bacteria associated with a UTI.Radiopaque calcium stones form because of an abundance of calcium in the blood as the result of excessive bone reabsorption secondary to immobility, bone disease, or renal tubular acidosis. Uric acid stones develop in acidic urine secondary to conditions such as gout, thiazide diuretic use, or a high-purine diet. Unlike calcium stones, they are not radiopaque and thus do not show up on x-ray.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


