myelin sheath that is often much thicker than the axon itself. The membrane of the axon is the membrane that actually conducts the action potential which is a change that spreads rapidly along the nerve fiber membrane.8 In order for both depolarization and repolarization of the nerve membrane to occur during the action potential, voltage-gated sodium channel play a role. A voltage-gated potassium channel also plays an important role in increasing the rapidity or repolarization of the membrane. These two voltage-gated channels are in addition to the Na+ – K+ pumps.8
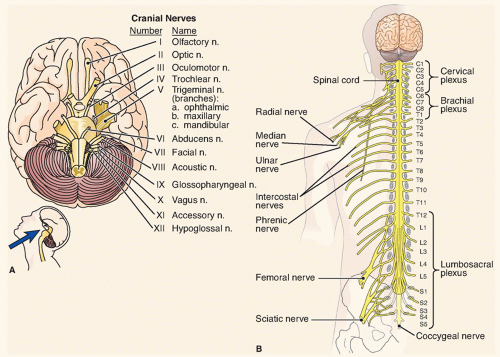 Figure 35-1 ▪ Peripheral nervous system. (A) The cranial nerves. (B) The spinal nerves and peripheral nerve plexuses. (From: McConnell, T. H. (2007). The nature of disease pathology for the health professions, Philadelphia: Lippincott Williams & Wilkins.) |
Anatomic involvement or distribution: single or multiple peripheral nerves, symmetric or asymmetric, proximal or distal involvement
Cause: infections, inflammation, vascular compromise, entrapment, disease entities (e.g., DM), alcohol abuse, vitamin deficiency, immune system disorders, toxic substances, and others
Pathologic process: wallerian degeneration, segmental demyelination, or distal axonal degeneration
Time frame of development: acute, subacute, chronic
Clinical presentation: presenting signs and symptoms including functional losses related to motor, sensory, autonomic, or mixed nerve changes
Genetic inheritance or mutations
as “dying forward,” a process in which the nerve degenerates from the point of axonal damage outward.6 The myelin and axon degeneration result in a loss of ability to transmit electrical impulses effectively. Regrowth may occur proximal to the transection, but it is slow and often incomplete, and recovery of the nerve is limited. Axonal degeneration refers to distal axonal breakdown resembling wallerian degeneration. However, the degeneration is caused from metabolic changes within neurons (e.g., DM, toxins). The myelin sheath and axon break down in a process that begins at the most distal part of the nerve fiber and progresses proximally toward the nerve cell body; this process is referred to as “dying-back.”
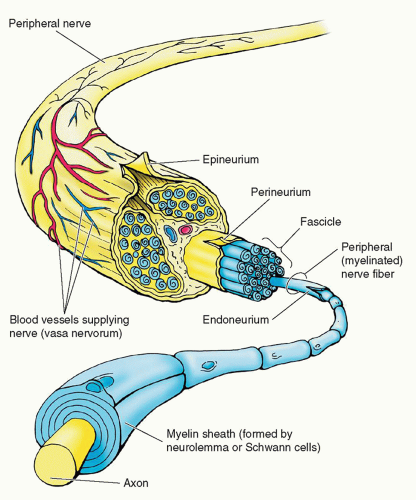 Figure 35-2 ▪ Arrangement and sheathment of peripheral, myelinated nerve fibers. All but the smallest peripheral nerves are arranged in bundles (fascicles), and the entire nerve is surrounded by the epineurium, a connective tissue sheath. Each small bundle of nerve fibers is also enclosed by a sheath-the perineurium. Individual nerve fibers have a delicate connective tissue covering-the endoneurium. The myelin sheath is formed by neurolemma (Schwann) cells. (From: Moore, K. L., & Dalley, A. F. II, (1999). Clinical oriented anatomy (4th ed.). Baltimore,: Lippincott Williams & Wilkins.) |
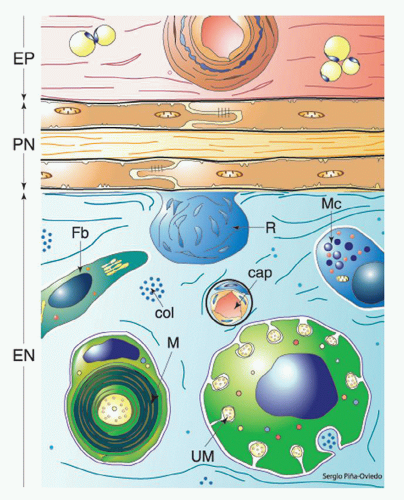 Figure 35-3 ▪ Diagram of the major elements of peripheral nerve compartments. The epineurium (EP) contains collagen, blood vessels, and some adherent adipose tissue. The flattened cells of the perineurium (PN) are joined by tight junctions and form flattened layers separated by collagen fibers. Renaut bodies (R) project into the endoneurium (EN). Schwann cells forming lamellated myelin (M) (drawn uncompacted in this diagram) surround the larger axons. Multiple unmyelinated axons (UM) are invaginated into the surface of Schwann cells. Other elements include fibroblasts (Fb), mast cells (Mc), capillaries (cap), and collagen (col). (From: Mills, S. E. (2007) Histology for pathologists (3rd ed.). Philadelphia: Lippincott Williams & Wilkins.) |
TABLE 35-1 CATEGORIES AND ETIOLOGIES OF PERIPHERAL NEUROPATHIES | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
TABLE 35-2 CLASSIFICATION OF PERIPHERAL NEUROPATHIES BASED ON PROXIMAL TO DISTAL | ||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||
Does the history/physical examination suggest localized peripheral nerve involvement?
Is there any evidence of hereditary neuropathy?
Have detailed past, family, medical, occupational, and drug histories been collected?
Have all symptoms been fully described and accounted for?
Is the neuropathy focal, multifocal, or generalized?
What is the involvement of motor, sensory, and autonomic involvement?
What diagnostics might be helpful?
What pattern of signs and symptoms has unfolded?
Are associated medical conditions evident?
weakness, what is the distribution of weakness? Evidence of upper motor neuron involvement is also considered. In both the sensory and motor examination, the examiner is also interested in determining any patterns of altered sensory or motor loss such as symmetrical or asymmetrical and focal versus multifocal patterns of dysfunction and the time frame for development. Reflexes are evaluated. Any autonomic dysfunctions are also noted.
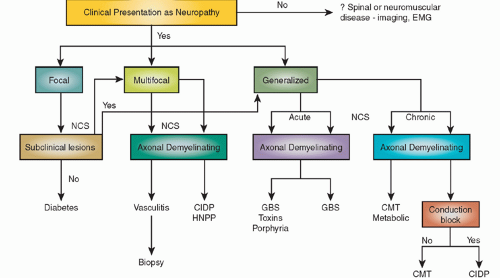 Figure 35-4 ▪ Algorithm for stepwise approach to assessing and investigating a possible neuropathy. CIDP, chronic inflammatory demyelinating polyneuropathy; CMT, Charcot-Marie-Tooth disease; EMG, electromyography; GBS, Guillain-Barre syndrome; NCS, nerve conduction study; HNPP, hereditary neuropathy with liability to pressure palsies. (From: Figure 1 from Willison, H. J., & Winer, J. B. (2003). Clinical evaluation and investigation of neuropathy. Journal of Neurology, Neurosurgery, & Psychiatry, 74(2), ii3-ii8.) |
lower extremities resulting in balance dysfunction.20 Diabetic peripheral neuropathy is caused by microvascular abnormalities resulting in nerve damage.
Distal, symmetric, mostly sensory polyneuropathy affecting feet and legs greater than hands that progresses slowly (most common)
Acute diabetic ophthalmoplegia (affects third and sometimes CN VI) unilaterally
Acute mononeuropathy of limbs or trunk including a painful thoracolumbar radiculopathy
Acute/subacute evolving, painful asymmetric, mostly motor neuropathy that affects the upper lumbar roots and proximal leg muscles
Symmetric proximal motor weakness and wasting often without pain and with variable sensory loss pursuing a subacute or chronic course
Autonomic neuropathy with bowel, bladder, and circulatory reflexes
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


