Reed, C., Carroll, L., Baccari, S., et al. (2011). Spica cast care: A collaborative staffled education initiative for improved patient care. Orthopaedic Nursing, 30(6), 353-358.
Young, S., Fevang, J. M., Gullaksen, G., et al. (2010) Deformity and functional outcome after treatment for supracondylar humerus fractures in children: A 5- to 10-year follow-up of 139 supracondylar humerus fractures treated by plaster cast, skeletal traction or crossed wire fixation. Journal of Child Orthopedics, 4, 445-453.
Casting, bracing, and splinting are all means of immobilizing an injured or diseased body part. The length of time can vary from a few days to several months, depending on the nature of the problem. The management of children who are immobilized differs little from that of the adult; however, age-appropriate changes must be considered. See Procedure Guidelines 54-1, pages 1744 to 1745.
Complications of Immobilization
Peripheral neurovascular compromise.
Alteration in skin integrity due to pressure or friction.
Loss of efficient use of affected extremity due to noncompliance.
Traction
Traction is the application of a pulling force to an injured or diseased part of the body or an extremity while a counter traction pulls in the opposite direction. Traction may be used to reduce fractures or dislocations, maintain alignment and correct deformities, decrease muscle spasms and relieve pain, promote rest of a diseased or injured body part, and promote exercise. Advances in nailing and rodding, especially external fixators for fractures and spinal curvatures, have reduced the use of traction in many centers. See Procedure Guidelines 54-2, pages 1745 to 1751.
Types of Traction
Manual—direct pulling on the extremity or body part. Usually used to reduce fractures before treatment or immobilization.
Skin—force is applied directly to the skin by means of traction strips or tapes secured by elastic bandages or by means of traction boots. Usually of short-term duration and commonly used in children in whom small amounts of force are required.
Skeletal—force is applied to the body part through fixation directly into or through bone by means of a traction pin or screw. Allows for greater force over longer periods or used when skin traction is not feasible, as in soft tissue injury or damage.
Continuous or intermittent—traction forces should be disrupted only in accordance with the health care provider’s orders.
PROCEDURE GUIDELINES 54-1
Care of the Child with a Cast, Splint, or Brace
EQUIPMENT
• Casting materials or immobilization device
• Cotton padding material, plastic padding
PROCEDURE
Nursing Action
Rationale
1.
Prepare child for the procedure by showing materials to be used and describing procedure in age-appropriate terms.
1.
Reduces fear and enlists cooperation.
2.
Assess the need for pain medication, sedation, distraction techniques, or restraint and administer, as ordered.
2.
Manipulation of the affected part may be painful, so pharmacologic preparation is usually necessary.
3.
Obtain baseline neurovascular assessment, including discoloration or cyanosis, impaired movement, loss of sensation, edema, absent pulses, and pain disproportionate to injury or not relieved by analgesics.
3.
Will serve as a baseline to compare subsequent assessments after immobilization.
4.
Assist with application of the immobilization device.
5.
Help facilitate drying of a cast or splint.
Keep the child and affected part still until dry.
Support the curves of the cast with pillows.
Avoid excessive handling of the cast, and use palms when handling it.
5.
About 24 to 48 hours are required for drying a plaster cast. Dries from the outside inward, so may appear dry but is still moldable with movement or pressure.
6.
Assess the skin around edges of the device daily for signs of skin irritation. Teach child or parents to look for and report redness, skin breakdown, localized pain, foul odor that may indicate open wounds under device.
6.
Pressure or friction may disrupt skin integrity. May be readily visible or occur under the device and not detected until advanced. Braces can be altered if skin irritation becomes apparent.
7.
Try to prevent skin breakdown by padding edges of device and telling child to avoid placing anything inside the device.
7.
Avoids friction or pressure damage to skin and underlying tissue.
8.
Assess neurovascular status frequently after application of device, then daily to detect compromise.
8.
Initial swelling from the injury may contribute to vascular insufficiency or nerve compression.
9.
If child is in hip-spica cast, prevent skin breakdown from frequent soiling around perineum.
Line cast edges around the perineum with a plastic covering to prevent soiling of cast.
Use a fracture bedpan or urinal to facilitate toileting.
If not toilet trained, use a small diaper or perineal pad tucked under the edges of the cast, covered by a larger diaper, and change diapers as soon as soiled.
Wash the perineum frequently and dry thoroughly.
9.
Soiled edges of the cast may contribute to skin irritation or begin to disintegrate.
e.
If the cast is synthetic and becomes soiled, clean it with a damp cloth and small amount of detergent.
e.
Plaster casts cannot be washed because they absorb water and soften.
Cast removal
1.
Prepare the child for cast removal by describing the sensation (warmth, vibration) and demonstrating the cast cutter by touching it lightly to your palm.
1.
Children are frightened by the loud noise and believe that the cast cutter will cut through their skin or extremity.
2.
Provide and teach care of skin after cast, brace, or splint removal.
2.
An accumulation of dead skin and sebaceous secretions causes the skin to appear brown and flaky.
a.
Wash with soapy warm water.
b.
Soak the area daily with warm water to facilitate removal of desquamated skin and secretions.
c.
Advise child to avoid scratching; instead apply lotion or oil to relieve itching.
c.
Excessive rubbing may cause trauma.
d.
Encourage exercise as prescribed to regain strength and function.
d.
May initially be weak and stiff due to lack of use.
PROCEDURE GUIDELINES 54-2
Care of a Child in Traction
EQUIPMENT
• Traction tapes
• Elastic bandages
• Spreader blocks, ropes, weights, pulleys
• Adhesive tape
• Tincture of benzoin/other adhesive agent
• Traction bars, slings
PROCEDURE
Nursing Action
Rationale
1.
Explain the procedure to the child and parents.
1.
If the traction is to be effective, it is essential that the parents and child understand traction.
2.
Maintain even, constant traction.
2.
Traction must be kept constant to achieve the desired results.
a.
Do not add or remove weights unless ordered.
b.
Allow the weights to hang free at all times.
c.
Be certain that the ropes are in the wheel grooves of the pulleys.
c.
Maintains proper alignment.
d.
Keep the weights out of the child’s reach.
d.
Prevents loosening or undoing of traction knots.
e.
Wrap knotted areas of the ropes with adhesive tape to prevent slipping.
f.
Do not elevate the head or foot of the bed without consulting health care provider.
f.
May disrupt traction forces.
g.
Supervise the child’s position so that the purpose of the traction is accomplished.
3.
Check for disturbance of circulation by observing:
3.
Compares the affected extremity with the unaffected one.
a.
Skin color—for redness, pallor, cyanosis.
a.
May indicate neurovascular compromise.
b.
Joint motion restriction.
c.
Skin temperature—warmth.
d.
Tingling, numbness.
e.
Swelling, edema.
4.
Provide skin care.
4.
Immobilized children readily develop areas of pressure unless meticulous skin care is provided.
a.
Pad bony prominences (ankles) with cotton padding before wrapping with elastic bandages.
a.
Protects skin from injury.
b.
Wash and dry all exposed areas thoroughly.
c.
Massage the child’s back and sacral area frequently, using lotion.
c.
Stimulates microcirculation and acts as a lubricant.
d.
Inspect the heels, ankles, popliteal space, and top of the foot for signs of pressure from elastic bandages.
d.
These are the areas most prone to breakdown.
e.
Keep the linen free from wrinkles and food crumbs.
e.
Prevents undue pressure areas.
f.
Do not allow the traction cords to dig into child’s skin.
f.
This is a safety measure.
g.
Use a fracture bedpan.
g.
This is less awkward and more comfortable for the child.
5.
Plan for short periods of muscle exercise every day.
Encourage use of unaffected extremity.
Assist the child to exercise unaffected joints.
Provide for diversionary activities that require movement of unaffected joints and muscles.
5.
Disuse of muscles can result in atrophy, contractures, and deformities.
6.
Encourage deep-breathing exercises.
6.
Prevents respiratory complications of prolonged immobilization.
7.
Record intake and output.
7.
Prolonged immobilization renders the child prone to urine retention and renal calculi.
8.
Encourage a diet high in fiber and fluids.
8.
Helps to prevent constipation and urinary calculi.
9.
Provide daily diversion and encourage visitation from family and friends.
9.
Helps prevent boredom and assists the child to cope with immobilization.
a.
Suspend or place favorite toys within easy reach of child.
b.
Provide for continuing education for school-age children.
b.
Length of immobilization in traction may be considerable.
c.
Encourage activities that will allow for diversion: drawing, coloring, video games.
c.
Activities that can be done while remaining in traction.
d.
Immobilized patients should be roomed together, if possible.
d.
Encourages peer support.
10.
If not contraindicated, provide the child with an overhead trapeze.
10.
This will assist with movement and self-help.
11.
Document the following:
11.
Proper documentation facilitates communication between health care providers.
a.
Color, temperature, and appearance of the affected limb.
Foot of bed may need to be raised or placed on “shock blocks” to prevent child from being pulled to foot of bed.
a.
Frequently the child’s weight is insufficient to maintain proper alignment of the extremity.
13.
Do not alter the traction system.
13.
Notify the health care provider if adjustment is indicated.
14.
Avoid sudden movement or jarring of bed.
14.
This can cause pain to the child and disturb alignment.
15.
Do not allow weights to hang over the child’s bed.
15.
This is a safety precaution.
Skin traction
1.
Do not apply over an open wound or over damaged skin.
1.
The skin must be intact for the pull of the traction to be effective. Prevents contamination of the wound and further skin breakdown.
2.
Prepare the skin with an adhesive agent before application of traction tapes.
2.
Adhesive agents allow the traction tapes to adhere better, preventing friction on the skin surface.
Skeletal traction
1.
Treat all entry sites as surgical wounds.
1.
Reduces the chance of infection along the pin or screw tract.
a.
Clean entry site according to your facility’s policy or guidelines. This should be done at least once per shift.
a.
Policies vary. Cleaning the pin site prevents infection, promotes comfort by preventing skin from adhering to pin.
b.
Assess the entry site every shift for indications of infection or slippage.
b.
Notify health care provider if either of these conditions exists.
2.
Protect the exposed ends of skeletal traction pins.
2.
Protects the health care provider as well as the child from injury.
Specific traction types
Bryant’s traction
Indications
To reduce fractures of the femur in children younger than age 2 or weighing less than 30 lb (14 kg).
Also used to stabilize the hip joint when casting is not indicated.
Preoperatively to attempt reduction of a developmentally dislocated hip in the same age group.
Mechanism of action
Involves the bilateral vertical extension of the child’s legs. The child’s weight serves as the countertraction. Skin traction is applied to both limbs to minimize potential trauma and maintain stability and alignment of child.
Bryant’s traction.
1.
Maintain appropriate position:
1.
Proper positioning is needed to achieve desired results.
a.
The legs are extended at right angles to the body.
b.
The hips are elevated slightly from the bed.
c.
The buttocks are elevated slightly from the bed.
c.
Ensures proper traction pull.
d.
The heels and ankles are free from pressure.
d.
Prevents skin breakdown.
2.
Check condition and position of elastic bandages every shift. Rewrap, as indicated and permitted by the health care provider.
2.
Elastic bandages can cause compression and compromise circulation. In addition, force across skin surfaces needs to be constant and free from constriction to prevent skin breakdown and ensure adequate traction force.
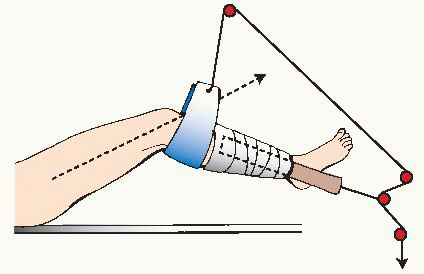
Russel’s traction(see figure at right)
Indications
Reduces fractures of the femur or hip.
Treatment of specific types of knee injuries or contractures.
Mechanism of action
Traction force is applied to the limb through application of skin traction. This can be accomplished with traction tapes or a traction boot in older individuals.
Russel’s traction.
1.
Application of elastic bandages:
Wrap bandages from ankle to thigh on patients younger than age 2.
Older patients should have bandages wrapped from ankle to the knee.
1.
Proper application of the tapes prevents neurovascular compromise and ensures proper and adequate pull on the extremity.
2.
Place foot support against both feet.
2.
Prevents footdrop.
3.
Keep the heel free from the bed.
3.
Prevents pressure sores and ensures continuous traction pull.
4.
Carefully assess the popliteal space for signs of pressure from the knee sling.
4.
Prevents pressure sores or neurovascular compression.
5.
Assess the neurovascular status of limb at least every 2 hours.
5.
Early detection can prevent injury to patient.
6.
Make sure that the footplate or spreader block is wide enough.
6.
Prevents pressure sores and circulatory compromise.
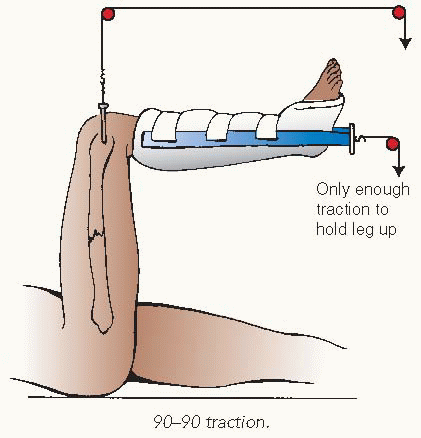
90-degree-90-degree traction (90-90)(see figure at right)
Indications
Reduces fractures of the femur when skin traction is inadequate.
Mechanism of action
Traction force is applied through skeletal traction pin placed through the distal femur. A short leg cast or foam boot may be used to help suspend the lower leg. Traction force is applied to femur only through pin. Only enough weight should be used to hold lower limb suspended.
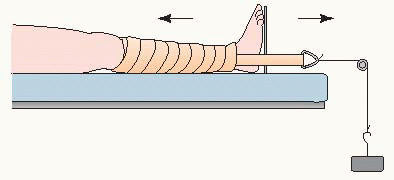
Buck’s extension(see figure at right)
Used to correct or prevent knee and hip contractures, to rest the limb, to prevent spasm of injured muscles or joints, or to temporarily immobilize a fractured limb.
Mechanism of action
The traction force is delivered through a traction boot or skin traction in a straight line.
Buck’s extension.
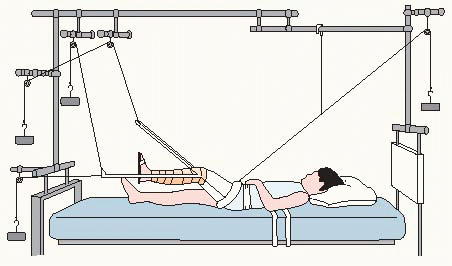
Balanced suspension with Thomas splint and Pearson attachment(see figure at right)
Indications
Occasionally still used in older children and adolescents for fractured femurs to rest an injured lower extremity or joint.
Mechanism of action
Thomas splint suspends the thigh; Pearson attachment applied to the splint allows knee flexion and supports the leg below the knee.
Balanced suspension.
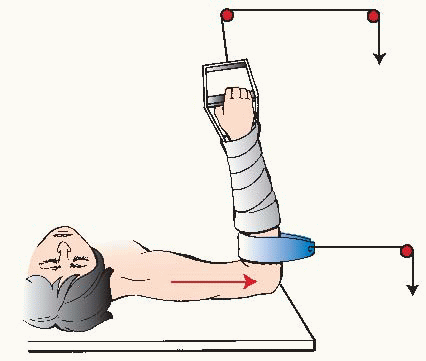
Dunlop’s traction (overhead 90-90)(see figure at right)
Indications
Used to treat fractures of the humerus and injuries in or around the shoulder girdle.
Mechanism of action
Traction force is applied usually through skin traction on the upper arm only. Occasionally, skeletal traction through an olecranon screw or pin in the distal humerus may be indicated. The lower arm is held in balanced suspension only. The elbow is maintained at 90 degrees of flexion or slightly more.
Dunlop’s traction.
1.
Make sure that the traction tapes are properly adhered and wrapped.
1.
Prevents damage to the skin and ensures proper pull.
2.
Assess the neurovascular status of the extremity every 2 hours.
2.
Elastic bandages can cause circulatory or neurologic compromise. Early detection can prevent patient harm.
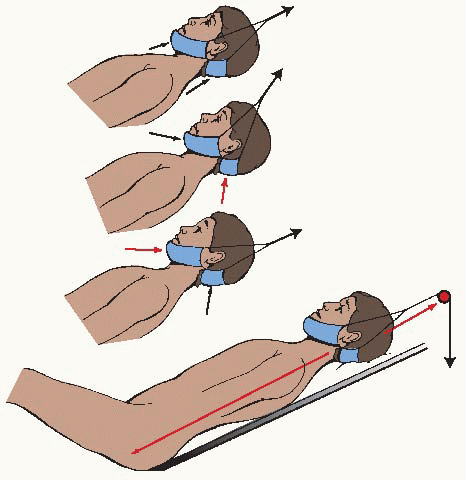
Cervical traction(see figures at right)
Indications
Used for stabilization of spinal fractures or injuries, muscle spasms, muscle contractures.
Mechanism of action
Traction force applied through a head halter (skin traction) or directly to the skull by means of Crutchfield tongs or halo apparatus.
Cervical traction.
1.
Head halter must be assessed for proper positioning. It should not place pressure on ears, skin, or throat.
1.
Prevents pressure sores.
2.
Maintain flat bed position.
2.
Proper spinal alignment is critical to prevent further injury.
3.
Keep the child in proper position and alignment.
4.
Crutchfield tongs or halo pin sites should be treated as skeletal traction sites.
4.
Prevents infection.
Halo-femoral traction
Indications
Used to correct severe spinal curvatures either before surgery or after a spinal release before final correction.
Mechanism of action
A halo is affixed to the skull. A traction pin is placed in each distal femur. Traction force is applied upward to the halo and downward to the femurs, pulling the spine into alignment.
1.
General traction considerations must be followed. The child is usually placed on a Stryker frame or special bed.
1.
Allows for more accessible care of the immobilized patient.
2.
Assess the child carefully every 2 hours for any increased complaints of pain, respiratory difficulty, or nerve injury.
2.
Complaints should not be ignored because alteration in any of these can indicate neurologic or spinal injury. Notification of health care provider is vital to prevent further harm.
3.
Be alert for symptoms of injury to cranial nerves:
Lateral gaze paralysis.
Difficulty in swallowing.
Difficulty in coughing.
Voice changes.
Tongue weakness.
3.
Common cranial nerve injuries:
Abducens nerve palsy (most common injury).
Vagus nerve.
Vagus nerve.
Glossopharyngeal nerve.
Hypoglossal nerve.
4.
Be alert for symptoms of injury to spinal cord:
Weakness, numbness in legs.
Loss of bladder function.
Upturning or downturning of toes.
Clonus of ankles or knees.
4.
These complaints may indicate lower spinal nerve root or cauda equina damage and should be reported promptly.
5.
Be alert for symptoms of brachial plexus injuries:
Difficulty in moving hand, shoulder, or arm.
Numbness or weakness in hand.
5.
These complaints or findings may be caused by impingement on spinal nerves.
6.
Assess all pin sites for loosening every shift.
6.
Loose pins can cause harm to the child as well as prevent proper traction pull. Halo-gravity traction, using the child’s body and gravity as counterweights, may be used instead of pins.
7.
Keep the torque wrench for the halo pins at the bedside at all times.
7.
The halo or pins may have to be removed or adjusted in an emergency or to ensure proper tension on the pins.
Complications of Traction
Neurovascular compromise to extremity.
Skin and soft tissue injury.
Pin or screw tract infection, osteomyelitis (with skeletal traction).
COMMON ORTHOPEDIC DISORDERS IN CHILDREN
Fractures
A fracture is a break or disruption in the continuity of bone. Fractures in children differ from those in adults due to the differences in anatomy, biomechanics, and physiology of the child’s skeleton compared to that of an adult. Involvement of the epiphysis or metaphysis can disrupt the epiphyseal plate, interfering with growth (see Figure 54-1). Fractures are extremely common in children, with an estimated 42% of boys and 27% of girls sustaining fractures during childhood.
Evidence Base
Abzug, J., & Zlotolow, D. (2012). Pediatric hand and wrist fractures. Current Orthopaedic Practice, 23(4), 327-330.
Sponsellar, P. (2011). Handbook of pediatric orthopedics. New York: Thieme.
Pathophysiology and Etiology
Most fractures in children are a result of low-velocity trauma such as a fall.
Up to age 2, most fractures are sustained as a result of the child being injured by another person.
Fractures in neonates and infants are commonly the result of child maltreatment. Child maltreatment should be suspected when treating fractures in this age group.
A bone fractures when the force applied to it exceeds the amount the bone can absorb.
Children’s long bones are more resilient than those of adults. They are able to withstand greater deflection without fracturing.
Children’s bones also have thick periosteum.
Figure 54-1. Structure of a bone.
The involvement of growth plates (epiphyseal plate) is unique to fractures in children. Cartilaginous growth plates are present at each end of the long bones and at one end of metacarpals and metatarsals. The plate is weaker than surrounding ligaments, tendons, and joint capsules and is disrupted before these tissues are injured.
Damage to the growth plate may result in cessation of or a disturbance in bone growth (depending on the extent of damage sustained at the growth plate).
On the other hand, acceleration in bone growth commonly occurs after a fracture in the long bones of children.
Children’s fractures heal more rapidly than adult fractures. The younger the child, the more rapidly bone heals.
Children’s fractures remodel more completely and actively than adult fractures and usually result in less disability and deformity.
Sites of Fractures in Children
Evidence Base
Gourde, J., & Damian, F. (2012). ED fracture pain management in children. Journal of Emergency Nursing, 38(1), 91-97.
Woratanarat, P., Angsanuntsukh, C., Rattanasiri, S., et al.. (2012). Meta-analysis of pinning in supracondylar fracture of the humerus in children. Journal of Orthopedic Trauma, 26, 48-53.
As children grow, the fracture rate increases, with the peak incidence occurring in early adolescence. Forearm fractures are the most common injury.
Forearm and Wrist Fractures
Most common site of fracture in children, with most occurring in children older than age 5.
Major categories of classification include fracture dislocations, midshaft fractures, and distal fractures.
Most common cause is from a fall on an outstretched arm.
Epiphyseal or Growth Plate Injuries
Constitutes approximately 15% to 25% of all skeletal injuries in children.
The most frequent site of physeal injuries (excluding phalangeal fractures) is the distal radius and ulna.
The 11- to 15-year-old age group tends to sustain the majority of physeal injuries to the distal radius and ulna.
The mechanism of injury is usually a fall on an outstretched arm.
Clavicle Fractures
Frequent site of fracture in children.
The shaft of the clavicle is the most common site of injury.
A fall on the shoulder or excessive lateral compression of the shoulder is usually the mechanism of injury.
Treatment involves support in the form of immobilization with a sling.
Reduction of clavicle fractures in children occurs only in instances of extreme displacement.
Humerus Fractures
The mechanism of injury for the majority of humeral fractures is a fall onto an outstretched arm or hand.
Supracondylar fractures are the most common fractures of the humerus; they may be associated with acute vascular injury.
Approximately 10% of all humeral fractures occur at the shaft of the humerus; they are usually a result of twisting injuries in infants and toddlers. Direct trauma to the humeral shaft is the most common mechanism of injury in older children.
Distal humeral fractures occur more often in the lateral epicondyle than the medial epicondyle.
Less than 1% of fractures occur at the proximal humerus.
Spinal Fractures
Rare in children.
Mechanism of injury is due to significant trauma, such as a motor vehicle accident, fall from a significant height, athletic activities, beatings, or pedestrian-motor vehicle accident.
Most spinal fractures involve the cervical spine.
Pelvic Fractures
Pelvic fractures are uncommon in children and adolescents; they are commonly the result of high-energy trauma or a crush-type injury.
Associated injuries are present in approximately 75% of children with pelvic fractures and include hemorrhage and damage to the abdominal wall and pelvic organs.
Hip Fractures
Hip fractures in children are uncommon, but may occur from motor vehicle accidents, bicycle accidents, falls from significant heights, or child maltreatment (in children under age 3).
Hip fractures can result in avascular necrosis of the femoral head and damage to the physis resulting in growth arrest, malunion, and nonunion.
Pelvic avulsion fractures are more common, especially in boys ages 12 to 14.
Femur Fractures
Common in children. Peak incidence occurs in two age groups—children ages 2 to 3 and adolescents.
Femoral shaft (diaphysis) fractures are the most common location.
Usually the result of high-energy trauma, such as a motor vehicle accident or fall from a significant height; most common cause in children younger than age 1 is child maltreatment.
Tibial Fractures
The most common lower extremity fracture in children occurs in the tibial and fibular shaft—constitutes 10% to 15% of all pediatric fractures.
Most diaphyseal tibia fractures in children ages 5 to 6 are nondisplaced or minimally displaced spiral or oblique fractures. A rotational mechanism of injury to the lower leg is the most common cause of tibial fractures in children under age 3 (toddler’s fracture or CAST [childhood accidental spiral tibial]).
Greater force is required to injure the tibia in older children; motor vehicle accidents and sports injuries are the most common causes of tibial fractures in children and adolescents.
Ankle Fractures
Common in children and adolescents—approximately 5% of all pediatric fractures.
Involve the growth plate in approximately every one of six injuries.
Greatest incidence is in males ages 10 to 15.
Usually the result of direct trauma.
Mortise view as well as anteroposterior (AP) and lateral x-rays should be obtained.
Foot Fractures
Foot fractures account for approximately 6% of all fractures in children and 50% of foot fractures occur at the metatarsals.
Most metatarsal and phalangeal fractures are nondisplaced.
Mechanism of injury is usually a direct or indirect trauma, such as from falls, jumping from heights, object falling on foot, and twisting injuries.
Classification of Fractures
Open fractures: underlying fracture in bone communicates with an external wound; usually the result of high-energy trauma or penetrating wounds.
Closed fractures: underlying fracture with no open wound.
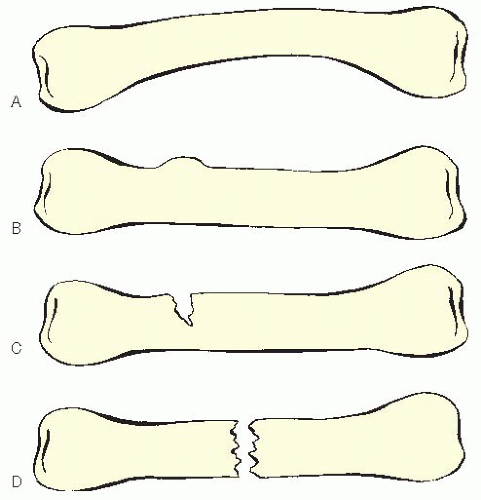
Plastic deformation: a bending of the bone in such a manner as to cause a microscopic fracture line that does not cross the bone. When the force is removed, the bone remains bent. Unique to children and most common in the ulna (see Figure 54-2A).
Buckle (torus) fractures: fracture on the tension side of the bone near the softer metaphyseal bone; crosses the bone and buckles the harder diaphyseal bone on the opposite side, causing a bulge (see Figure 54-2B).
Figure 54-2. Common fractures in children. (A) Plastic deformation (bend). (B) Buckle (torus). (C) Greenstick. (D) Complete.
Greenstick fracture: bone is bent and the fracture begins but does not entirely cross through the bone (see Figure 54-2C).
Only gold members can continue reading. Log In or Register to continue
 Evidence Base
Evidence Base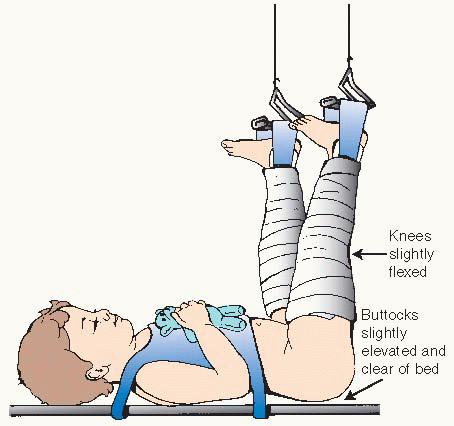
 Evidence Base
Evidence Base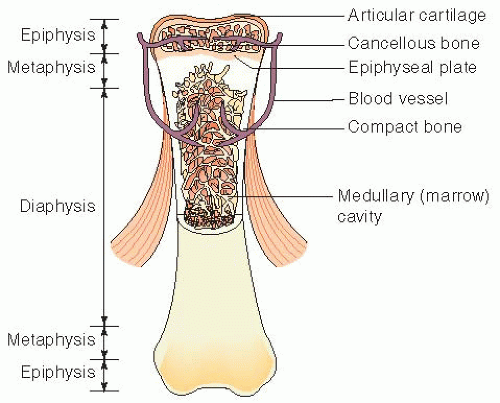
 Evidence Base
Evidence Base