Pain is a multidimensional experience characterized by physiologic and psychological components. It is a complex phenomenon that involves both perception of a stimulus and response to it. One third of cancer patients in active therapy and 60% to 90% of patients with advanced disease have pain. One critically important aspect related to the definition of pain is to understand that it is subjective. Cancer pain is unique in many ways. Patients can have pain in more than one site, it can have more than one cause, and patients can have more than one syndrome. In addition, they can have acute and chronic pain simultaneously, and the pain can vary in its pattern, intensity, and duration. As a result of its multiple causes and presentation, cancer pain often requires more than one treatment. The patient’s perception of pain and the subsequent self-report are the most reliable measures that health care providers should use to assess and control pain successfully.
A. Types of Pain
1.Nociceptive pain occurs when nociceptors are activated by noxious stimulus (eg, injury, disease).
a.Somatic pain is the most common type of pain and can occur in cutaneous or deep tissues (eg, with bone metastases).
b.Visceral pain is another type of nociceptive pain (eg, distention of the liver capsule and the intestinal viscera).
2.Neuropathic pain occurs as a result of injury to nerves (eg, tumor infiltrating the brachial plexus, chemotherapy-induced peripheral neuropathies).
B. Classification of Pain
1.Acute pain is characterized as a “complex, unpleasant experience with emotional and cognitive, as well as, sensory features that occur in response to tissue trauma.” It is usually nociceptive and associated with subjective and objective physical signs and activation of the autonomic nervous system. The cause of the pain is usually known (Chapman & Nakamura, 1999).
2.Chronic pain continues after an injury is healed. It may be nociceptive, neuropathic, or both. Hyperactivity of the autonomic nervous system is less common. Patients may not “appear” to be in pain.
3.Cancer pain can be caused by the disease (eg, tumor invasion, compression of nerves) or by treatment or procedures (eg, biopsy, chemotherapy, surgery). It can have features of nociceptive pain, neuropathic pain, or both. It can be acute or chronic in nature.
Preliminary pain assessment data are obtained. This includes a brief history, physical examination, laboratory data, and pain intensity information.
Patient comfort is maximized with prompt administration of analgesics. This facilitates the evaluation process.
Mild pain is usually treated with nonopioids, whereas the opioid analgesics are used for moderate to severe pain.
The oral route of administration is preferred for virtually all patients.
Analgesics with short half-lives are used to facilitate rapid dose escalation and prompt relief of pain.
Analgesics are given “around the clock” rather than “as needed.”
Once baseline opioid requirements are determined, sustained-release opioid preparations can be used to reduce the number of pills taken each day.
PRN medications are available for breakthrough pain.
A prophylactic bowel regimen is initiated with all opioid therapy. Nausea and vomiting are treated with aggressive antiemetic therapy. These may become less prominent after the first several days of opioid therapy.
The dose of each analgesic is maximized before considering changes in drugs or routes of administration.
Changes in analgesics or routes of administration are generally based on the development of significant toxicities that are not responsive to usual measures rather than the total administered dose.
Equi-analgesic tables are used to approximate opioid dose conversions.
Serial pain intensity ratings are obtained and documented in the medical record.
A comprehensive pain assessment is completed as outlined in the text.
The treatment approach and diagnoses are reassessed based on the results of the pain assessment and relief scores.
The potential benefits and risks of the following approaches to pain management are assessed.
Antineoplastic therapies
Adjuvant analgesics
Neurostimulatory techniques
Nonpharmacologic approaches
Regional anesthesia
Neuroablative procedures
Consider referral to an experienced multidisciplinary pain team if attempts to control pain in patients with the following difficult-to-manage problems are not successful.
Patients with neuropathic pain
Patients with episodic or incident pain
Patients with impaired cognitive or communicative function
1. Problems related to health care professionals (eg, inadequate knowledge of pain management, incomplete assessment, fear of addiction)
2. Problems related to patients (eg, reluctance to report pain, fear that pain means disease is worse, reluctance to take pain medicines because of fear of addiction and side effects)
3. Problems related to the health care system (eg, pain a low priority, access to pain treatments, costs of treatment, and restrictive regulations of controlled substances)
II. Etiology:
Table 30-2 lists common cancer pain syndromes from all causes.
A. Disease-related causes (ie, tumor that has infiltrated bones, nerves, and viscera) are the most common reason for cancer pain. Tumor-related causes can be both acute and chronic in nature.
*Examples of common pain syndromes unrelated to cancer: Lumbar or cervical disk disease, migraine.
Adapted from Grossman, S., & Gregory, R. (1996). Pain. In J. Kirkwood, M. Lotze, & J. Yasko (Eds.), Current cancer therapeutics (2nd ed., p. 374). Philadelphia: Current Medicine.
B. Treatment-related causes include those brought on by procedure, diagnostic methods, surgery, chemotherapy, and radiation. These causes can also be either acute or chronic in nature.
C. Causes unrelated to cancer or its treatment account for the smallest percentage of pain in cancer patients. However, it is important for the clinician to differentiate between cancer- and non-cancer-related causes, because the treatments may be very different.
III. Patient Management
A. Assessment: The following are physical indications of pain:
1. Facial grimacing
2. Moaning
3. Guarding
4. Increased heart and respiratory rates
5. Increased blood pressure
B. Diagnostic Parameters: A comprehensive assessment is conducted for a new pain or a significant change in an existing pain. A simpler assessment, such as asking a patient about current pain intensity and degree of relief, is warranted before and after administering an analgesic. Pain assessment is of particular importance in patients who have communication difficulties (eg, non-English speaking, children, and the elderly). The frequency of assessment is directly related to the success of adequate pain control. The following are essential pain assessment parameters:
1. Assessment of pain intensity and character
a. Onset and temporal character: When did it start? How often does it occur?
b. Location: Where is it?
c. Quality: What does it feel like? (stabbing, shooting, cramping, dull, aching)
d. Intensity: What is the intensity of current pain?
(1) Numerical rating scale: On a scale of 0 to 10, with 0 being no pain and 10 being the worst pain imaginable, ask the patient to select a number between 0 and 10 that best describes the pain.
(2) Verbal descriptor scale: Ask the patient to indicate if he or she is in pain. If so, ask if the pain is mild, moderate, or severe.
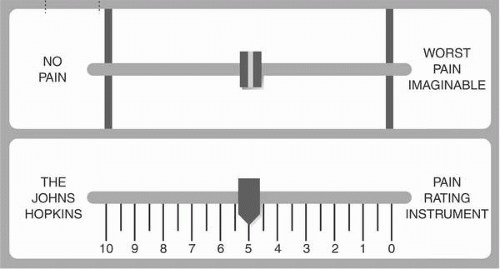
(3) Hopkins Pain Rating Instrument (a plastic, portable, 10-cm, double-sided instrument): Show the patient the side that contains no numbers but has “no pain” on one end and “worst pain imaginable” on the other. Ask the patient to slide the plastic tab to the place that represents the pain. Look at the reverse side of the instrument to see the numerical rating of the pain (Fig. 30-1).
2. Aggravating and relieving factors: What makes the pain better or worse?
a. Previous treatment: What treatments were used in the past and how successful were they?
b. Relief from current treatment: Is relief of pain complete, almost complete, partial, very little, or none?
c. Side effects of current treatment: Are you experiencing any side effects to current treatment?
Figure 30-1. The Johns Hopkins Pain Rating Instrument. The upper panel shows the front side of the instrument; the lower panel shows the back. Thus, when the tab is at “the worst pain imaginable” rating (front), the score reads “10” (back).
3. Assess psychosocial factors.
a. Effect of pain on patient and family members
b. Meaning of pain to patient and family
c. Usual coping strategies for pain and other stressors
d. Mood states
e. Effect of pain on sleep and fatigue
f. Concern about addiction and side effects of medication
g. Concern about costs of treatment
4. Diagnostic tests are performed to determine the causes of pain and aid in selection of the most appropriate intervention. Performing physical and neurologic examinations and ordering and reviewing diagnostic tests are the responsibility of the physician or primary provider. Tests should be appropriate to the body area and function, and to the possible etiology of the pain.
C. Treatment: The administration of analgesics is one of the most common nursing activities to help control pain. The nurse must possess adequate knowledge about analgesic pharmacology.
1. Categories of analgesics
a. Nonopioids (for mild/moderate pain): Have a peripheral mechanism of action; have a ceiling effect; are used alone or in combination with opioids. They include acetaminophen, aspirin, nonsteroidal antiinflammatory drugs (NSAIDs), and COX-2 inhibitors (Tables 30-3, 30-4, 30-5, 30-6, 30-7)
b. Opioids (for moderate/severe pain): Have a central mechanism of action; do not have a ceiling effect; are given on a scheduled basis with prn for breakthrough pain. Most patients have successful management with the oral route. (See Tables 30-4, 30-5, 30-6, 30-7, 30-8 and Box 30-1 for general comments, side effects, and routes of administration.)
TABLE 30-3 Adult Dosing Data for Nonopioids
Acetaminophen
650 mg q4h 975 mg q6h
APAP lacks the peripheral antiinflammatory and antiplatelet activities of the other NSAIDs.
Aspirin
650 mg q4h 975 mg q6h
The standard against which other NSAIDs are compared. May inhibit platelet aggregation for >1 week and may cause bleeding. Aspirin is contraindicated in children with fever or other viral disease because of its association with Reye’s syndrome.
Carprofen
100 mg tid
Choline magnesium trisalicylate
1000-1500 mg tid
May have minimal antiplatelet activity.
Choline salicylate
870 mg q3-4h
May have minimal antiplatelet activity.
Diclofenac
50-75 mg q12-24h
Diflunisal
500 mg q12h
Etodolac
200-400 mg q6-8h
Fenoprofen
300-600 mg q6h
Flubiprofen
50-100 mg q12h
Ibuprofen
400-600 mg q6h
Indomethacin
25-50 mg q6-8h
Ketoprofen
25-60 mg q6-8h
Ketorolac tromethamine
PO 10 mg q4-6h (maximum dose 40 mg/day)
Duration of use not to exceed 5 days
IM: 60 mg initially, then 30 mg q6h
IV: 30 mg initially, then 15 mg q6h
Magnesium salicylate
650 mg q4h
Meclofenamate sodium
50-100 mg q6h
Coombs’-positive autoimmune hemolytic anemia has been associated with prolonged use.
Mefenamic acid
250 mg q6h
Meloxicam
7.5-15 mg q24h
Nabumetone
500 mg q24h
Naproxen
250-275 mg q6-8h
Naproxen sodium
275 mg q6-8h
Phenylbutazone
100 mg q8h
Piroxicam
10-20 mg q24h
Sodium salicylate
325-650 mg q3-4h
Sulindac
150-200 mg q12-24g
Tolmetin
400-800 mg q8h
COX-2 Inhibitors
Celecoxib
100-200 mg q12h
Rofecoxib
12.5-25 mg q24h
Valdecoxib
10 mg q24h
Grossman, S. A. (1999). Management of cancer pain: National comprehensive cancer network guidelines. Oncology, 13, 33-44; American Pain Society. (1999). Principles of analgesic use in the treatment of acute pain and chronic cancer pain: A concise guide to medical practice (4th ed.) Glenview, IL: Author; Jacox, S., Carr, D., Payne, R., et al. (1994). Management of cancer pain: Clinical practice guideline No. 9 (AHCPR Publication No. 94-0592; p. 48). Rockville, MD: Agency for Health Care Policy and Research, U.S. Dept. of Health and Human Services.
TABLE 30-4 Routes of Administration
Route
Definition and Notes
Drug Types
Comments
Oral
By mouth (per os) Requires functioning GI tract, intact swallowing mechanism, sufficient GI tract for absorption to occur
Nonopioids, opioids, adjuvant analgesics
Advantages: convenient, noninvasive, cost-effective, flexible, less discomfort than injections with comparable efficacy Disadvantages: requires functional GI system; slow onset of action and relatively delayed peak effects; requires patient compliance
Rectal
Insertion of suppository into rectum
Nonopioids, opioids
Useful in patients who cannot take medications by mouth Any opioid may be compounded for rectal administration
Intramuscular
Injection into large muscle (e.g., gluteus or vastus lateralis)
Some nonopioids, opioids
IM administration should not be used, especially for chronic treatment, due to multiple disadvantages:
Painful injections
Wide fluctuations in drug absorption make it difficult to maintain consistent blood levels
Rapid fall-off of action compared with PO administration
Chronic injections may damage tissue (fibrosis, abscesses); IV and SC injections are appropriate alternatives
Intravenous
Injection into vein; may be single or repetitive bolus or continuous infusion with or without PCA
Some nonopioids, opioids, adjuvant analgesics
IV is most efficient ROA for immediate analgesia and permits rapid titration IV bolus produces rapid onset of effect, but shorter duration of action than IM; not recommended for drugs with long half-lives Continuous IV infusion provides steadier drug blood levels, which maximize pain relief while minimizing side effects
Subcutaneous
Placement of drug just under skin with small needle Continuous SC infusion can be obtained with a small needle
Some opioids
Advantages: produces steady blood levels; time until onset of effect is comparable to IM administration and effects are longer lasting, with less painful administration; cheaper than IV administration; obviates need for GI function Disadvantages: slower onset and offset and lower peak effects than IV administration, time consuming, often disliked by patients
Topical
Applied directly to the skin, where the drug penetrates
NSAIDs, local anesthetics (eg, lidocaine patch and gel, EMLA), capsaicin
Advantages: local effect (ie, no significant serum levels) limits side effects to local reactions, no drug-drug interactions; easy to use, no titration needed Disadvantages: may cause local skin reactions
Transdermal
Absorbed through skin with gradual release into the systemic circulation
Some opioids, adjuvant analgesics
Advantages: convenient, noninvasive, provides prolonged, relatively stable analgesia Disadvantages: delayed onset of action with first dose, drug absorption influenced by internal or external heat
Oral transmucosal
Delivery of drug to mouth, including sublingual (under tongue) and buccal/gingival administration
Some opioids
Advantages: easy, requires little staff supervision; avoids significant liver metabolism associated with oral opioids Disadvantages: variable absorption, bitter taste, dose is limited
OTFC
Fentanyl incorporated into a sweetened matrix on a stick for consumption
Fentanyl
Some absorption by way of oral mucosa, but most by way of GI tract; yields higher drug levels and better bioavailability than oral fentanyl
Intranasal
Small aerosol device placed inside nostril that delivers a calibrated dose of a drug
Butorphanol, sumatriptan
Takes advantage of rich blood supply to nose and also avoids significant liver metabolism associated with some drugs
Intraspinal
Epidural and intrathecal administration
Other (sublingual, vaginal)
Placement of drug under the tongue (sublingual) or in the vagina
Opioids
Most opioids can be absorbed sublingually or vaginally in patients who have problems such as impaired swallowing, short gut syndrome, or poor IV access
EMLA: Eutectic Mixture of Local Anesthetics (lidocaine and prilocaine); GI: gastrointestinal; IM: intramuscular; IV: intravenous; NSAIDs: nonsteroidal antiinflammatory drugs; OTFC: oral transmucosal fentanyl citrate; PCA: patient-controlled analgesia; PO: per os (oral); ROA: route of administration; SC: subcutaneous.
Berry P. H., Chapman C. R., Covington E. C., et al, (2001). Pain: Current understanding of assessment, management, and treatments. Reston VA: National Pharmaceutical Council and the Joint Commission for Accreditation of Healthcare Organizations.
Only gold members can continue reading. Log In or Register to continue