1. A broad term that encompasses functional and degenerative changes in the gastrointestinal (GI) system, resulting in inflammation, epithelial tissue sloughing, and ulceration.
2. The GI tract is affected in its entirety, but the term mucositis is most often used to describe oral mucosal injury.
3. The severity of mucositis can affect the course of treatment and the patient’s quality of life.
4. Incidence ranges from 10% of patients receiving adjuvant chemotherapy to 89% of blood and marrow transplantation patients. Average of approximately 35% to 40% incidence of mucositis with antineoplastic therapy
5. Toxicity may be severe enough to require a chemotherapy or radiotherapy dose reduction or delay in the next treatment cycle.
II. Etiology
A. Pathophysiology
1. The oral mucosa is an injury-sensitive but rapidly regenerating tissue that can be damaged by multiple stressors in cancer patients.
a. The outer epithelial layer is replaced every 7 to 14 days.
b. The short life cycle of these cells is primarily responsible for their increased sensitivity to the stresses of cancer therapy.
2. Saliva contains enzymes that protect the oral mucosa from dryness and infection. Decreased production of saliva enhances the risk of mucositis.
3. Indirect toxic effects in the mouth by the release of inflammatory mediators
4. The mouth has diverse and complex microflora that cause infection of damaged tissues. Recent studies have not shown a decrease in mucositis in patients using antimicrobial lozenges.
5. Altered nutritional status impedes the body’s ability to regenerate healthy tissue.
6. Mucositis is more prevalent in younger people, thought to be related to a more rapid epithelial cell turnover rate
B. The most common etiologic factors for mucositis are listed in Table 29-1.
TABLE 29-1 Etiologies and Physiologic Mechanisms of Mucositis
Chemotherapy prevents immediate regeneration of mucosal membranes, resulting in a peak incidence of mucositis occurring 2-14 days after initiation of cancer therapy. Type of chemotherapy with highest association to mucositis.
Chemotherapy prevents immediate regeneration of mucosal membranes, resulting in a peak incidence of mucositis occurring 2-14 days after initiation of cancer therapy. Direct injury from chemotherapy secreted in saliva (eg, methotrexate) may also induce epithelial damage.
Antimicrobials
Erythromycin
Broad-spectrum antimicrobials destroy the normal protective flora of the mouth, increasing the risk of fungal superinfection (esp. Candida).
Antitumor antibiotics
Actinomycin D Bleomycin sulfate Dactinomycin Daunorubicin Doxorubicin Epirubicin Idarubicin Mithramycin Mitomycin C Mitoxantrone
Chemotherapy prevents immediate regeneration of mucosal membranes, resulting in a peak incidence of mucositis occurring 2-14 days after initiation of cancer therapy.
Biologic response modifiers—cytokines
Interferon Interleukin-2 Tumor necrosis factor
Biologic therapy produces mucositis beginning 2-5 days after initiation of therapy and lasting 7-10 days after the treatment is complete. Forty percent of patients receiving cytokines develop mucositis.
Biologic response modifiers—antibodies
Gemtuzumab
Poorly defined specific features
Graft-versus-host disease (GVHD)
Acute GVHD Chronic GVHD
Severe mucositis occurs in 80% of blood and marrow transplant patients 2 or more weeks after transplantation.
The mechanism of injury is thought to be T-lymphocytic infiltration of normal epithelial tissue.
Mucositis presents in a significant number of individuals.
Chronic GVHD after allogeneic bone marrow transplant causes fibrotic changes in skin and mucous membranes that result in hyposalivation and a risk of oral infection that may also cause mucositis.
Hepatic disease
Hyperammonemia increases bleeding risk, mucosal changes, and taste alterations. High urea levels increase bleeding risk, alter mucosal integrity, and cause taste alterations.
Leads to an excessive amount of ammonia in saliva, causing spontaneous bleeding of gums, gray exudate, and complaints of a salty metal taste. Dry mouth with taste changes precede mucosal breakdown.
Mechanical irritation
Endotracheal tubes Ethanol Frequent oral suction Orogastric tubes Smoking and other tobacco products
Oral irritation in the location of the tube or suction can cause injury ranging from mild to hemorrhagic. Reducing the strength of suction can decrease the severity of oral injury.
Miscellaneous anti-neoplastic agents
L-asparaginase Trimetrexate
Chemotherapy prevents immediate regeneration of mucosal membranes, resulting in a peak incidence of mucositis occurring 4-10 days after initiation of therapy.
Miscellaneous nonchemo-therapeutic agents
Menogaril
Neutropenia
Depth of aplasia increases risk of mucositis.
Preexisting WBC abnormalities and prolonged neutropenia associated with hematologic malignancies and HIV disease lead to three to seven times higher incidence of mucositis than in other patient groups
Prolonged neutropenia (>10 days) increases risk of mucositis.
Other disorders interfering with WBC function (eg, diabetes mellitus, renal dysfunction, hepatic dysfunction, autoimmune disease)
Nutritional deficiencies
Intake of high-calorie, high-sugar foods to maintain body weight, but also enhance oral bacterial growth.
Insufficient fluid uptake leads to dry and vulnerable oral mucosa.
Plant alkaloids
Etoposide (high doses) Vinblastine Vinorelbine
Chemotherapy prevents immediate regeneration of mucosal membranes, resulting in a peak incidence of mucositis occurring 7-14 days after initiation of therapy.
Periodontal disease (preexisting)
Caries and caries-associated periapical pathology increase the risk of infection-related mucositis.
The preexisting bacterial load of the oral cavity causes oral infection when the patient becomes neutropenic or immunocompromised.
Abnormal oral bites, oral bridges, and dentures.
Poor oral hygiene enhances proliferation of oral microbes.
Phenytoin causes gingival hyperplasia, along with gum tenderness and a greater risk of injury.
Candida albicans infection is the most common infection, and herpes simplex virus is second in prevalence.
Ulcerative mucositis places the patient at risk for streptococcal bacteremia.
Radiation therapy
One hundred percent of patients receiving radiation to the neck area have mucositis.
Peak incidence within second week of therapy, or after 2,000 cGy has been administered.
Taxanes
Paclitaxel Docetaxel
Chemotherapy prevents immediate regeneration of mucosal membranes, resulting in a peak incidence of mucositis occurring 7-14 days after initiation of therapy.
Xerostomia
Radiation therapy to the head and neck region is a common etiology.
a. The onset of mucositis begins right after chemotherapy; however, the symptoms peak 7 to 10 days after therapy.
b. The period of greatest mucosal damage correlates with the white cell nadir.
c. The areas of the mouth that are most susceptible to mucosal damage are the soft tissues of the soft palate, floor of the mouth, tongue, and buccal mucosa.
2. Signs and symptoms of mucositis
a. Oral pain often precedes mucositis development. The pain is often a burning sensation.
b. Dry mouth (xerostomia) and thick, ropy saliva are often associated with the early stages of mucositis.
c. Oral erythema is the result of epidermal cell sloughing and the capillaries being closer to the skin surface.
d. Oral edema occurs at the edges of the tongue and along the left and right buccal mucosa.
e. Pseudomembranes are whitish coverings over the oral mucosa, with tender erosive tissue beneath the surface. Pseudomembranes may or may not be painless but often reflect the location where ulcerations will occur.
f. Ulcerations are shallow abrasions involving the entire epithelial tissue layer. They are common along the teeth line, the buccal mucosa, the lip mucosa, the floor of the mouth, and the ventral surface of the mouth. When severe ulceration occurs, hypersalivation is a more common presentation.
B. Diagnostic Parameters
1. There are no serum or urine tests used to diagnose or indicate the presence of mucositis; however, the presence of neutropenia or thrombocytopenia may exacerbate the clinical manifestations of mucositis.
2. Oral assessment is the only way to diagnose the presence of mucositis.
a. Although many assessment tools are available, none has shown a clear advantage over another.
b. The main objective of assessment is to perform consistent and ongoing observation of the oral cavity.
c. Mucositis is rated as mild, moderate, or severe based on numeric scores compiled from findings in all areas of the mouth.
d. Assessment scales
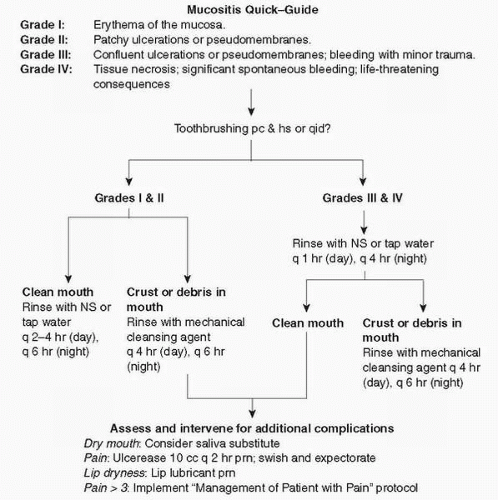
(1) A simple and easy-to-use oral assessment scale derived from the World Health Organization (WHO) scale is used in the National Cancer Institute’s (NCI) Common Toxicity Index version 3.0 (Fig. 29-1).
(2) Oral Mucositis Assessment Scale (OMAS) was created by a multidisciplinary work group of experts for research on mucositis (Sonis et al., 1999). This tool was determined valid and reliable in a multicenter study, and highly correlated with the NCI scoring system.
(3) Oral Mucositis Index (OMI) is a 34-question index for dental professionals; however, it has been recently converted to OMI-20 for nondental health professionals. The OMI-20 is a valid and reliable tool for rating mucositis (McGuire et al., 2002).
(4) Oral Assessment Guide (OAG) is an “oral cavity assessment tool,” not just a mucositis tool. The user evaluates eight parameters, grading them as normal, somewhat abnormal, and severely abnormal. The parameter totals are calculated to create a numeric score and grading of mucositis as absent or mild, moderate, and severe (Eilers, 2003).
e. The components of the oral examination are universal regardless of whether a research-based assessment instrument is used. (A sample assessment procedure can be found in Table 29-2.)
f. Common features of abnormal assessment findings are noted in Table 29-3.
C. Treatment
1. There are no specific therapies to prevent mucositis.
2. Mucositis is treated primarily symptomatically with oral cleansing, rinsing, topical agents, and pain medication.
3. Therapy breaks or dose restrictions of antineoplastic therapy can prevent mucositis recurrence or reduce severity in future treatment cycles.
Figure 29-1. Oral care algorithm. (Johns Hopkins Oncology Center)
4. There is a plethora of studies in the literature using common and unusual treatments to prevent and reduce severity of mucositis.
a. An overview of some of these agents is included in Table 29-4.
b. The U. S. Food and Drug Administration (FDA) has approved two drugs for prevention or treatment of xerostomia: pilocarpine and amifostine.
D. Nursing Diagnoses
1. Altered mucous membranes related to radiation therapy, chemotherapy, graft-versus-host disease, infection, trauma, medications, altered nutrition, and altered health maintenance
a.Problem: Damage to rapidly dividing epithelial tissues leads to altered tissue integrity, discomfort, and increased risk of infection. Oral mucosal injury occurs approximately 7 to 14 days after antineoplastic chemotherapy, and at other times when related to other etiologic factors.
TABLE 29-2 Oral Assessment Procedure
Steps of the Oral Assessment Procedure
Implications of Clinical Findings
Explain to the patient that the oral cavity will be inspected for overall hygiene and mucositis.
Patient cooperation can be maximized when they are well informed.
Turn on overhead lights and don gloves.
Promotes visualization
Gather supplies:
Implements assist in optimal visualization
Tongue blade
Light source
Gauze
Ask the patient to rate oral cavity pain at the time of assessment. If the oral examination is normal but pain is present, this must be noted.
If oral pain is greater than 3 on a 10-point scale, protocol for pain management is initiated, and more detail about the oral discomfort should be described.
The patient often at first describes a mucosal “burning” sensation.
The pain is usually continuous and exacerbated by mouth care, swallowing, and sleeping (due to mouth breathing).
Other common descriptors patients use to describe mucositis pain are: tender, aching, and sharp.
Mouth pain is particularly difficult to control because it is difficult for patients to swallow pain medication. Hospital admissions can be attributed to mucositis pain and dehydration.
Inspect the lips. Note the following:
Note any moles, birthmarks, cracking or peeling, ulcerations, red marks, or edema.
All lip edges (inner and outer) intact?
Are lips smooth?
The lips are a relatively transparent layer of cells, not keratinized (horny) where evaporation occurs. Healthy lips are smooth with clear edges. Observe for presence of cheilitis or fissures and or white plaques at the corners of the mouth.
Are there moles or birthmarks?
Have patient open his or her mouth.
Facilitates visualization
Turn on the light source and look into the mouth.
Facilitates visualization
Observe dentition:
Note any broken or missing teeth, the fit of dentures, any decayed teeth, fractured teeth, or missing fillings. The crown portion of the tooth is above the gum line and covered with enamel dentin to create a shiny white appearance of a calcified substance. Pulp contains blood vessels and nerves; if there is decay reaching the pulp, it causes pain.
Are all teeth present?
If there are dentures, remove before performing oral examination.
Are any teeth fractured?
Are any teeth decayed?
Where are fillings and bridges? Do they appear intact?
Are teeth shiny and white? Note any debris on or between teeth.
Observe the gingivae.
Note if the gums are receded or hyperplastic. Redness along the line of dentition may indicate infection below the gum surface. Gums that bleed easily may indicate gingival infection, hormonal disturbance, or thrombocytopenia.
Observe if saliva is present (visually, or detected on the tongue blade used throughout the examination):
If the tongue blade sticks to the tongue’s surface, there is inadequate saliva. Thick and ropey saliva is also an indication of inadequate production. Both the absence of saliva and copious thick saliva can occur in the presence of mucositis. Assess the rest of the mouth and the inside of the lips for erythema, pseudomembranes (whitish overcoating), edema, lesions, and bleeding. Use a tongue blade to assess the buccal mucosa for lesions caused by the trauma of mastication. The mouth and the inside of the lips are lined with mucous membrane of stratified squamous nonkeratinized cells. The stratified layer protects the mouth from abrasive food.
Is it clear?
Is it thin and watery or thick and ropey?
Place the tongue blade on the buccal mucosa. Take tongue blade and place it between the gum line and buccal mucosal wall. Starting on the right side, and using the light to illuminate the oral cavity, look for erythema, swelling, lesions, or bleeding of the buccal mucosa. Repeat this procedure on the left side of the mouth.
Gently pull out the labial mucosa (lip mucosa) and observe.
The lips are very moisture dependent and are good indicators of oral health.
Shine the light into the center of the mouth and inspect the tongue.
Look for erythema, dry appearance, prominent papillae, or smooth papillae, signaling disease. Any discolorations or lesions should also be noted.
Have the patient lift the tongue, move it to the right, then to the left.
Use a light to inspect the floor of the mouth, the underside of the tongue, and the sides of the tongue.
The ventral side of the tongue and the floor of the mouth is an area often affected by mucositis.
If the patient is unable to lift the tongue, use a gauze on the tongue and a tongue blade against the buccal mucosa to lift the tongue, separate tissues, and visualize the area.
Using the light source, inspect the hard and soft palate. Press on the center of the tongue, and ask the patient to say “ah” while the tongue surface is held down with a tongue blade to assist in visualizing the soft palate and uvula.
Assess dysphagia by determining the patient’s ability to swallow liquids and solid foods.
Dysphagia indicates mucositis in the posterior oropharynx. One study demonstrated an alarming incidence of “silent” aspiration in head and neck cancer patients with radiation induced mucositis (Eisbruch et al., 2002).
Assess voice.
Interpret loss of voice as a possible indication of the severity of mucositis in the esophagus. Loss of voice indicates severe edema around the vocal cords and should alert the health care provider to prepare to artificially maintain the airway.
Only gold members can continue reading. Log In or Register to continue