nursing responsibilities during labor and birth, including ways to provide comfort and support.
A look at labor and birth
Labor and birth is physically and emotionally straining for a woman. As the patient’s body undergoes physical changes to help the fetus pass through the cervix, she may also feel discomfort, pain, panic, irritability, and loss of control. To ensure the safest outcome for the mother and child, you must fully understand the stages of labor as well as the factors affecting its length and difficulty. With an understanding of the labor and birth process, you’ll be better able to provide supportive measures that promote relaxation and help increase the patient’s sense of control.
Fetal presentation
Fetal presentation is the relationship of the fetus to the cervix. It can be assessed through vaginal examination, abdominal inspection and palpation, sonography, or auscultation of fetal heart tones. By knowing the fetal presentation, you can anticipate which part of the fetus will first pass through the cervix during delivery.
How long and how hard
Fetal presentation can affect the length and difficulty of labor as well as how the fetus is delivered. For example, if the fetus is in a breech presentation (the fetus’s soft buttocks are presenting first), the force exerted against the cervix by uterine contractions is less than it would be if the fetus’s firm head presented first. The decreased force against the cervix decreases the effectiveness of the uterine contractions that help open the cervix and push the fetus through the birth canal.
Presenting difficulties
Sometimes, the fetus’s presenting part is too large to pass through the mother’s pelvis or the fetus is in a position that’s undeliverable. In such cases, cesarean birth may be necessary. In addition to the usual risks associated with surgery, an abnormal fetal presentation increases the risk of complications for the mother and fetus.
Factors determining fetal presentation
The primary factors that determine fetal presentation during birth are fetal attitude, lie, and position.
Fetal attitude
Fetal attitude (degree of flexion) is the relationship of the fetal body parts to one another. It indicates whether the presenting parts of the fetus are in flexion (complete or moderate) or extension (partial or full).
What’s in an attitude?
Complete flexion
Moderate flexion
Partial extension
Full extension
In complete flexion, the head of the fetus is tucked down onto the chest, with the chin touching the sternum.
Moderate flexion (aka military position or sinciput), the head of the fetus is slightly flexed but held straighter than in complete flexion. The chin doesn’t touch the chest.
In partial extension, the head of the fetus is extended, with the head pushed slightly backward so that the brow becomes the first part of the fetus to pass through the pelvis during birth.
In complete extension, the head and neck of the fetus are hyperextended and the occiput touches the fetus’s upper back. The back is usually arched, which increases the degree of hyperextension.
This position is commonly called the fetal position.
Many fetuses assume this attitude early in labor but convert to complete flexion as labor progresses.
This is an uncommon fetal position and a vaginal birth is unlikely.
Commonly, this skull diameter is too large to pass through the pelvis.
The occiput is the presenting part.
The top of the head is the presenting part.
The brow or forehead is the presenting part.
The mentum (chin) is the presenting part.
Fetal lie
The relationship of the fetal spine to the maternal spine is referred to as fetal lie. Fetal lie can be described as longitudinal, transverse, or oblique.
Fetal position
Fetal position is the relationship of the presenting part of the fetus to a specific quadrant of the mother’s pelvis. It’s important to define fetal position because it influences the progression of labor and whether surgical intervention is needed.
Spelling it out
Fetal position is defined using three letters.
The first letter designates whether the presenting part is facing the woman’s right (R) or left (L) side. The second letter or letters refer to the presenting part of the fetus: the occiput (O), mentum (M), sacrum (Sa), or scapula or acromion process (A). The third letter designates whether the presenting part is pointing to the anterior (A), posterior (P), or transverse (T) section of the mother’s pelvis.
Commonly, the duration of labor and birth is shortest when the fetus is in the LOA or ROA position. When the fetal position is posterior, such as left occiput posterior (LOP), labor tends to be longer and more painful for the woman because the fetal head puts pressure on her sacral nerves. (See Determining fetal position.)
Which way do I Lie?
Longitudinal
Transverse
Oblique
The fetal spine is parallel to the maternal spine.
The fetal spine is at a 90-degree angle to the maternal spine.
The fetal spine is at a 45-degree angle to the maternal spine.
Approximately 99% of all fetuses are in this position. The presenting part can be either vertex or breech.
Occurs in less than 1% of all deliveries and is considered abnormal. The presenting part can be a shoulder, an iliac crest, a hand, or an elbow.
Also considered abnormal and is rare. The presenting part can also be a shoulder, an iliac crest, a hand, or an elbow.
Fetal position abbreviations
Here’s a list of presentations that are used when documenting vertex presentations. Although it is possible to apply the same abbreviation system to breech (sacrum), face (mentum) and shoulder (acromion process) presentation, it is rarely done due to those presentations precipitating a cesarean section delivery.
Vertex presentations (occiput)
LOA, left occipitoanterior
ROA, right occipitoanterior
LOP, left occipitoposterior
ROP, right occipitoposterior
LOT, left occipitotransverse
ROT, right occipitotransverse
Types of fetal presentation
Fetal presentation refers to the part of the fetus that presents into the birth canal first. It’s determined by fetal attitude, lie, and position. Fetal presentation should be determined in the early stages of labor in case an abnormal presentation endangers the mother and the fetus. (See Classifying fetal presentation, pages 300 and 301.)
The four main types of fetal presentation are:
cephalic
breech
shoulder
compound.
Cephalic presentation
When the fetus is in cephalic presentation, the head is the first part to contact the cervix and expel from the uterus during delivery. About 95% of all fetuses are in cephalic presentation at birth.
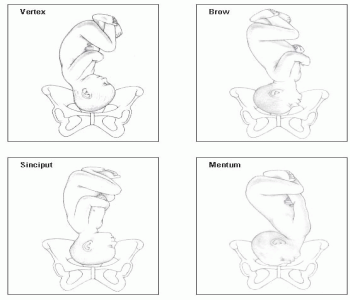
The four types of cephalic presentation are vertex, brow, face, and mentum (chin).
Determining fetal position
Fetal position is determined by the relationship of a specific presenting part (occiput, sacrum, mentum [chin], or sinciput [deflected vertex]) to the four quadrants (anterior, posterior, right, or left) of the maternal pelvis. For example, a fetus whose occiput (O) is the presenting part and who’s located in the right (R) and anterior (A) quadrant of the maternal pelvis is identified as ROA.
These illustrations show the possible positions of a fetus in vertex presentation.
Vertex
In the vertex cephalic presentation, the most common presentation overall, the fetus is in a longitudinal lie with an attitude of complete flexion. The parietal bones (between the two fontanels) are the presenting part of the fetus. This presentation is considered optimal for fetal descent through the pelvis.
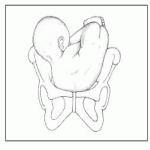
Classifying fetal presentation
Fetal presentation may be broadly classified as cephalic, shoulder, compound, or breech. Almost all births are cephalic presentations. Breech births are the second most common type.
Cephalic
In the cephalic, or head-down, presentation, the position of the fetus may be further classified by the presenting skull landmark, such as vertex, brow, sinciput, or mentum (chin).
Shoulder
Although a fetus may adopt one of several shoulder presentations, examination can’t differentiate among them; thus, all transverse lies are considered shoulder presentations.
Compound
In compound presentation, an extremity prolapses alongside the major presenting part so that two presenting parts appear in the pelvis at the same time.
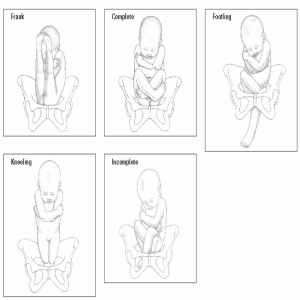
Breech
In the breech, or head-up, presentation, the position of the fetus may be further classified as frank, where the hips are flexed and knees remain straight; complete, where the knees and hips are flexed; kneeling, where the knees are flexed and the hips remain extended; and incomplete, where one or both hips remain extended and one or both feet or knees lie below the breech; or footling, where one or both feet extend below the breech.
Brow
In brow presentation, the fetus’s brow or forehead is the presenting part. The fetus is in a longitudinal lie and exhibits an attitude of partial flexion. Although this isn’t the optimal presentation for a fetus, few suffer serious complications from the delivery. In fact, many brow presentations convert to vertex presentations during descent through the pelvis.
Face
The face type of cephalic presentation is unfavorable for the mother and the fetus. In this presentation, the fetus is in a longitudinal lie and exhibits an attitude of complete extension. Because the face is the presenting part of the fetal head, severe edema and facial distortion may occur from the pressure of uterine contractions during labor.
Faced with potential complications
If labor is allowed to progress, careful monitoring of both the fetus and the mother is necessary to reduce the risk of compromise. Labor may be prolonged and ineffective in some instances, and vaginal birth may not be possible because the presenting part has a larger diameter than the pelvic outlet. Attempts to manually convert the face presentation to a more favorable position are rarely successful and are associated with high perinatal mortality and maternal morbidity.
Mentum
The mentum, or chin, type of cephalic presentation is also unfavorable for the mother and the fetus. In this presentation, the fetus is in a longitudinal lie with an attitude of complete extension. The presenting part of the fetus is the chin, which may lead to severe edema and facial distortion from the pressure of the uterine contractions during labor. The widest diameter of the fetal head is presenting through the pelvis because of the extreme extension of the head. If labor is allowed to progress, careful monitoring of both the fetus and the mother is necessary to reduce the risk of compromise. Labor is usually prolonged and ineffective. Vaginal delivery is usually impossible because the fetus can’t pass through the ischial spines.
Breech presentation
Although 25% of all fetuses are in breech presentation at week 30 of gestation, most turn spontaneously at 32 to 34 weeks’ gestation. However, breech presentation occurs at term in about 3% of births. Labor is usually prolonged with breech presentation because of ineffective cervical dilation caused by decreased pressure on the cervix and delayed descent of the fetus.
It gets complicated
In addition to prolonging labor, the breech presentation increases the risk of complications. In the fetus, cord prolapse; anoxia; intracranial hemorrhage caused by rapid molding of the head; neck trauma; and shoulder, arm, hip, and leg dislocations or fractures may occur. Complications that may occur in the mother include perineal tears and cervical lacerations during delivery and infection from premature rupture of the membranes.
How will I know?
A breech presentation can be identified by abdominal and cervical examination. The signs of breech presentation include:
fetal head is felt at the uterine fundus during an abdominal examination
fetal heart tones are heard above the umbilicus
soft buttocks or feet are palpated during a cervical examination.
Once, twice, three types more
The three types of breech presentation are complete, frank, and incomplete.
Complete breech
In a complete breech presentation, the fetus’s buttocks and the feet are the presenting parts. The fetus is in a longitudinal lie and is in complete flexion. The fetus is sitting crossed-legged and both legs are drawn up (hips flexed) with the anterior of the thighs pressed tightly against the abdomen; the lower legs are crossed with the calves pressed against the posterior of the thighs; and the feet are tightly flexed against the outer aspect of the posterior thighs. Although considered an abnormal fetal presentation, complete breech is the least difficult of the breech presentations.
Frank breech
In a frank breech presentation, the fetus’s buttocks are the presenting part. The fetus is in a longitudinal lie and is in moderate flexion. Both legs are drawn up (hips flexed) with the anterior of the thighs pressed against the body; the knees are fully extended and resting on the upper body with the lower legs stretched upward; the arms may be flexed over or under the legs; and the feet are resting against the head. The attitude is moderate.
Incomplete breech
In an incomplete breech presentation, also called a footling breech, one or both of the knees or legs are the presenting parts. If one leg is extended, it’s called a single-footling breech (the other leg may be flexed in the normal attitude); if both legs are extended, it’s called a double-footling breech. The fetus is in a longitudinal lie. At least one of the thighs and one of the lower legs are extended with little or no hip flexion.
Perhaps expect prolapse
A footling breech is the most difficult of the breech deliveries. Cord prolapse is common in a footling breech because of the space created by the extended leg. A cesarean birth may be necessary to reduce the risk of fetal or maternal mortality.
Shoulder presentation
Although common in multiple pregnancies, the shoulder presentation of the fetus is an abnormal presentation that occurs in less than 1% of deliveries. In this presentation, the shoulder, iliac crest, hand, or elbow is the presenting part. The fetus is in a transverse lie, and the attitude may range from complete flexion to complete extension.
Lacking space and support
In the multiparous woman, shoulder presentation may be caused by the relaxation of the abdominal walls. If the abdominal walls are relaxed, the unsupported uterus falls forward, causing the fetus to turn horizontally. Other causes of shoulder presentation may include pelvic contraction (the vertical space in the pelvis is smaller than the horizontal space) or placenta previa (the low-lying placenta decreases the vertical space in the uterus).
Early identification and intervention are critical when the fetus is in a shoulder presentation. Abdominal and cervical examination and sonography are used to confirm whether the mother’s abdomen has an abnormal or distorted shape. Attempts to turn the fetus may be unsuccessful unless the fetus is small or preterm. A cesarean delivery may be necessary to reduce the risk of fetal or maternal death.
Compound presentation
In a compound presentation, an extremity presents with another major presenting part, usually the head. In this type of presentation, the extremity prolapses alongside the major presenting part so that they present simultaneously.
Engagement
Engagement occurs when the presenting part of the fetus passes into the pelvis to the point where, in cephalic presentation, the biparietal diameter of the fetal head is at the level of the midpelvis (or at the level of the ischial spines). Vaginal and cervical examinations are used to assess the degree of engagement before and during labor.
A good sign
Because the ischial spines are usually the narrowest area of the female pelvis, an engagement indicates that the pelvic inlet is large enough for the fetus to pass through (because the widest part of the fetus has already passed through the narrowest part of the pelvis).
Floating away
In the primipara, nonengagement of the presenting part at the onset of labor may indicate a complication, such as cephalopelvic disproportion, abnormal presentation or position, or an abnormality of the fetal head. The nonengaged presenting part is described as floating. In the multipara, nonengagement is common at the onset of labor; however, the presenting part quickly becomes engaged as labor progresses.
Station
Station is the relationship of the presenting part of the fetus to the mother’s ischial spines. If the fetus is at station 0, the fetus is considered to be at the level of the ischial spines. The fetus is considered engaged when it reaches station 0.
Grand central stations
Fetal station is measured in centimeters. The measurement is called minus when it’s above the level of the ischial spines and plus when it’s below that level. Station measurements range from — 1 to — 3 cm (minus station) and + 1 to + 4 cm (plus station).
During a cervical examination, you’ll assess the extent of the fetal presenting part into the pelvis. This is referred to as fetal engagement.
After you have determined fetal engagement, palpate the presenting part and grade the fetal station (where the presenting part lies in relation to the ischial spines of the maternal pelvis). If the presenting part isn’t fully engaged into the pelvis, you won’t be able to assess station.
Station grades range from —3 (3 cm above the maternal ischial spines) to +4 (4 cm below the maternal ischial spines, causing the perineum to bulge). A zero grade indicates that the presenting part lies level with the ischial spines.
A look at labor stimulation
For some patients, it’s necessary to stimulate labor. The stimulation of labor may involve induction (artificially starting labor) or augmentation (assisting a labor that started spontaneously).
Although induction and augmentation involve the same methods and risks, they’re performed for different reasons. Many high-risk pregnancies must be induced because the safety of the mother or fetus is in jeopardy. Medical problems that justify induction of labor include preeclampsia, eclampsia, severe hypertension, diabetes, Rh sensitization, prolonged rupture of the membranes (over 24 hours), and a postmature fetus (a fetus that’s 42 weeks’ gestation or older). Augmentation of labor may be necessary if the contractions are too weak or infrequent to be effective.
Conditions for labor stimulation
Before stimulating labor, the fetus must be:
in longitudinal lie (the long axis of the fetus is parallel to the long axis of the mother)
at least 39 weeks’ gestation or have fetal lung maturity established
The ripe type
In addition to the above fetal criteria, the mother must have a ripe cervix before labor is induced. A ripe cervix is soft and supple to the touch rather than firm. Softening of the cervix allows for cervical effacement, dilation, and effective coordination of contractions. Using Bishop score, you can determine whether a cervix is ripe enough for induction. (See Bishop score, page 308.)
When it isn’t so great to stimulate
Stimulation of labor should be done with caution in women age 35 and older and in those with grand parity or uterine scars.
Labor should not be stimulated if, but not limited to:
transverse fetal position
umbilical cord prolapse
active genital herpes infections
women who have had previous myomectomy (fibroid removal) from the inside of the uterus
stimulation of the uterus increases the risk of such complications as placenta previa, abruptio placentae, uterine rupture, and decreased fetal blood supply caused by the increased intensity or duration of contractions.
Methods of labor stimulation
If labor is to be induced or augmented, one method or a combination of methods may be used. Methods of labor stimulation include breast stimulation, amniotomy, oxytocin administration, and ripening agent application.
Breast stimulation
In breast stimulation, the nipples are massaged to induce labor. Stimulation results in the release of oxytocin, which causes contractions that sometimes result in labor.
The patient or her partner can help with breast stimulation by:
applying a water-soluble lubricant to the nipple area (to prevent irritation)
gently rolling the nipple through the patient’s clothing.
Too much, too soon?
One drawback of breast stimulation is that the amount of oxytocin being released by the woman’s body can’t be controlled. In some cases (rarely), too much oxytocin leads to excessive uterine stimulation (tachysystole or tetanic contractions), which impairs fetal or placental blood flow, causing fetal distress.
Bishop score
Bishop score is a tool that you can use to assess whether a woman is ready for labor. A score ranging from 0 to 3 is given for each of five factors: cervical dilation, length (effacement), consistency, position, and station.
If the woman’s score exceeds 8, the cervix is considered suitable for induction.
Factor
Score
Cervical dilation
• Cervix dilated <1 cm
0
• Cervix dilated 1 to 2 cm
1
• Cervix dilated 2 to 4 cm
2
• Cervix dilated >4 cm
3
Cervical length (effacement)
• Cervical length >4 cm (0% effaced)
0
• Cervical length 2 to 4 cm (0% to 50% effaced)
1
• Cervical length 1 to 2 cm (50% to 75% effaced)
2
• Cervical length <1 cm (>75% effaced)
3
Cervical consistency
• Firm cervical consistency
0
• Average cervical consistency
1
• Soft cervical consistency
2
Cervical position
• Posterior cervical position
0
• Middle or anterior cervical position
1
Zero station notation (presenting part level)
• Presenting part at ischial spines —3 cm
0
• Presenting part at ischial spines —1 cm
1
• Presenting part at ischial spines +1 cm
2
• Presenting part at ischial spines +2 cm
3
Modifiers
Add 1 point to score for:
Preeclampsia
Each prior vaginal delivery
Subtract 1 point from score for:
Postdates pregnancy
Nulliparity
Premature or prolonged rupture of membranes
Adapted with permission from Bishop, E. H. (1964). Pelvic scoring for elective induction. Obstetrics and Gynecology, 24, 266-268.
Amniotomy
Amniotomy (artificial rupturing of the membranes) is performed to augment or induce labor when the membranes haven’t ruptured spontaneously. This procedure allows the fetal head to contact the cervix more directly, thus increasing the efficiency of contractions. Amniotomy is virtually painless for both the mother and the fetus because the membranes don’t have nerve endings.
System requirements
To perform amniotomy, the fetus must be in the vertex presentation with the cervix dilated to at least 2 cm; additionally, the head should be well applied to the cervix to help prevent umbilical cord prolapse. Nurse need to be aware of the potential for umbilical cord prolapse during an amniotomy if the head is not fully engaged into the pelvis at zero station.
Let it flow, let it flow, let it flow
During amniotomy, the woman is placed in a dorsal recumbent position. An amniohook (a long, thin instrument similar to a crochet hook) is inserted into the vagina to puncture the membranes. If puncture is properly performed, amniotic fluid gushes out.
Advice from the experts
Complications of amniotomy
Umbilical cord prolapse—a life-threatening complication of amniotomy—is an emergency that requires immediate cesarean birth to prevent fetal death. It occurs when amniotic fluid, gushing from the ruptured sac, sweeps the cord down through the cervix. Prolapse risk is higher if the fetal head isn’t engaged in the pelvis before rupture occurs. Cord prolapse can lead to cord compression as the fetal presenting part presses the cord against the pelvic brim. Immediate action must be taken to relieve the pressure and prevent fetal anoxia and fetal distress. Here are some options:
Insert a gloved hand into the vagina and gently push the fetal presenting part away from the cord.
Place the woman in Trendelenburg position to tilt the presenting part backward into the pelvis and relieve pressure on the cord.
Administer oxygen to the mother by face mask to improve oxygen flow to the fetus.
If the cord has prolapsed to the point that it’s visible outside the vagina, don’t attempt to push the cord back in. This can add to the compression and may cause kinking. Cover the exposed portion with a compress soaked with sterile saline solution to prevent drying, which could result in atrophy of the umbilical vessels.
Persevere if it isn’t clear
Normal amniotic fluid is clear. Bloody or meconium-stained amniotic fluid is considered abnormal and requires careful, continuous monitoring of the mother and fetus. Bloody amniotic fluid may indicate a bleeding problem. Meconium-stained amniotic fluid may indicate fetal distress. If the fluid is meconium-stained, note whether the staining is thin, moderate, thick, or particulate.
Take a whiff
Amniotic fluid has a scent described as either a sweet smell or odorless. A foul smell indicated the presence of an infection and the patient needs further evaluation.
Prolapse potential
Amniotomy increases the risk to the fetus because there’s a possibility that a portion of the umbilical cord will prolapse with the amniotic fluid. Fetal heart rate (FHR) should be monitored during and after the procedure to make sure that umbilical cord prolapse didn’t occur. (See Complications of amniotomy, page 309.)
Oxytocin administration
Synthetic oxytocin (Pitocin) is used to induce or augment labor. It may be used in patients with gestational hypertension, prolonged gestation, maternal diabetes, Rh sensitization, premature or prolonged rupture of membranes, and incomplete or inevitable abortion. Oxytocin is also used to evaluate for fetal distress after 31 weeks’ gestation and to control bleeding and enhance uterine contractions after the placenta is delivered.
Oxytocin is always administered I.V. with an infusion pump. Throughout administration, FHR and uterine contractions should be assessed, monitored, and documented according to National Institutes of Child Health and Human Development (NICHD) criteria.
First things first
Prior to the start of an infusion you should have at least a 15-minute strip of both FHR and uterine activity to establish a reassuring FHR. There also should be a Bishop score documented as a measure of ensuring the cervix is ripe for labor. Additionally, a set of maternal vital signs should also be obtained.
Nursing interventions
Here’s how to administer oxytocin:
Start a primary I.V. line.
Insert the tubing of the administration set through the infusion pump, and set the drip rate to administer the oxytocin at a starting infusion rate of 0.5 to 2 mU/minute. The maximum dosage of oxytocin is 20 mU/minute. Typically, oxytocin is diluted 10 units in 500 ml or 20 units in 1,000 ml of an isotonic solution; lactated Ringer is the most common. This dilution results in a dosage of 2 mU/minute for every 3 ml/hour of I.V. fluid infused. An alternative dosing is 30 units diluted in 500 ml and the dosage becomes 1 mU/minute for every 1 ml/hour of I.V. fluid infused.
Piggyback ride
The oxytocin solution is then piggybacked to the primary I.V. line, through the lowest possible access point on the I.V. tubing.
If a problem occurs, such as a nonreassuring FHR pattern or uterine tachysystole, stop the piggyback infusion immediately and resume the primary line.
Immediate action
Because oxytocin begins acting immediately, be prepared to start monitoring uterine contractions.
Increase the oxytocin dosage as ordered—but never increase the dose more than 1 to 2 mU/minute every 15 to 60 minutes. Typically, the dosage continues at a rate that maintains a regular pattern (uterine contractions occur every 2 to 3 minutes lasting less than 2 minutes duration).
If more is in store
Before each increase, be sure to assess contractions, maternal vital signs, fetal heart rhythm, and FHR. If you’re using an external fetal monitor, the uterine activity strip or grid should show contractions occurring every 2 to 3 minutes. The contractions should last for about 60 seconds and be followed by uterine relaxation. If you’re using an internal uterine pressure catheter (IUPC), look for an optimal baseline value ranging from 5 to 15 mm Hg. Your goal is to verify uterine relaxation between contractions.
Assist with comfort measures, such as repositioning the patient on her other side, as needed.
Following through
Continue assessing maternal and fetal responses to the oxytocin.
Maternal assessment should include blood pressure, pulse, and a pain assessment
To reduce uterine irritability, try to increase uterine blood flow. Do this by changing the patient’s position and increasing the infusion rate of the primary I.V. line. After tachysystole resolves, resume the oxytocin infusion per your facility’s policy.
Advice from the experts
Complications of oxytocin administration
Oxytocin can cause uterine tachysystole. This, in turn, may progress to tetanic contractions, which last longer than 2 minutes. Signs of tachysystole include contractions that are less than 2 minutes apart and last 90 seconds or longer, uterine pressure that doesn’t return to baseline between contractions, and intrauterine pressure that rises over 75 mm Hg.
What else to watch for
Other potential complications include fetal distress, abruptio placentae, uterine rupture, and water intoxication. Water intoxication, which can cause maternal seizures or coma, can result because the antidiuretic effect of oxytocin causes decreased urine flow.
Stop signs
Watch for the following signs of oxytocin administration complications. If any indication of any potential complications exists, stop the oxytocin administration, administer oxygen via face mask, and notify the doctor immediately.
Fetal distress
Signs of fetal distress include:
late decelerations
bradycardia.
Abruptio placentae
Signs of abruptio placentae include:
sharp, stabbing uterine pain
pain over and above the uterine contraction pain
heavy bleeding
hard, boardlike uterus.
Also watch for signs of shock, including rapid, weak pulse; falling blood pressure; cold and clammy skin; and dilation of the nostrils.
Uterine rupture
Signs of uterine rupture include:
sudden, severe pain during a uterine contractions
tearing sensation
absent fetal heart sounds.
Also watch for signs of shock, including rapid, weak pulse; falling blood pressure; cold and clammy skin; and dilation of the nostrils.
Water intoxication
Signs and symptoms of water intoxication include:
headache and vomiting (usually seen first)
hypertension
peripheral edema
shallow or labored breathing
dyspnea
tachypnea
lethargy
confusion
change in level of consciousness.
Ripening agent application
If a woman’s cervix isn’t soft and supple, a ripening agent may be applied to it to stimulate labor. Drugs containing prostaglandin E2 —such as dinoprostone (Cervidil, Prepidil, Prostin E2)—are commonly used to ripen the cervix. These drugs initiate the breakdown of the collagen that keeps the cervix tightly closed.
The ripening agent can be:
applied to the interior surface of the cervix with a catheter or suppository
applied to a diaphragm that’s then placed against the cervix
inserted vaginally.
Additional doses may be applied every 3 to 6 hours; however, two or three doses are usually enough to cause ripening. The woman should remain flat after application to prevent leakage of the medication.
Success half the time
The success of this labor stimulation method varies with the agent used. After just a single application of a ripening agent, about 50% of women go into labor spontaneously and deliver within 24 hours. Those women who don’t go into labor require a different method of labor stimulation.
Prostaglandin should be removed before amniotomy. Use this drug with caution in women with asthma, glaucoma, and renal or cardiac disease.
Not to be ignored
Prior to application of the ripening agent, a 15-minute strip of FHR and uterine activity should be completed as a baseline. Although the ripening agent is applied, carefully monitor the patient’s uterine activity. If uterine tachysystole occurs or if labor begins, the prostaglandin agent should be removed. The patient should also be monitored for adverse effects of prostaglandin application, including headache, vomiting, fever, diarrhea, and hypertension. FHR and uterine activity should be monitored continuously between 30 minutes and 2 hours after vaginal insertion, dependent upon the agent used.
Onset of labor
True labor begins when the woman has bloody show, her membranes rupture, and she has painful contractions of the uterus that cause effacement and dilation of the cervix. The actual mechanism that triggers this process is unknown.
Before the onset of true labor, preliminary signs appear that indicate the beginning of the birthing process. Although not considered to be a true stage of labor, these signs signify that true labor isn’t far away.
Preliminary signs and symptoms of labor
Preliminary signs and symptoms of labor include lightening, increased level of activity, Braxton Hicks contractions, and ripening of the cervix. Subjective signs, such as restlessness, anxiety, and sleeplessness, may also occur. (See Labor: True or false?)
Lightening
Lightening is the descent of the fetal head into the pelvis. The uterus lowers and moves into a more anterior position, and the contour of the abdomen changes. In primiparas, these changes commonly occur about 2 weeks before birth. In multiparas, these changes can occur on the day labor begins or after labor starts.
More pressure here, less pressure there
Lightening increases pressure on the bladder, which may cause urinary frequency. In addition, leg pain may occur if the shifting of the fetus and uterus increases pressure on the sciatic nerve. The mother may also notice an increase in vaginal discharge because of the pressure of the fetus on the cervix. However, breathing becomes easier for the woman after lightening because pressure on the diaphragm is decreased.
Advice from the experts
Labor: True or false?
Use this chart to help differentiate between the signs and symptoms of true labor and those of false labor.
Signs and symptoms
True labor
False labor
Cervical changes
Cervix softens and dilates
No cervical dilation or effacement
Level of discomfort
Intense
Mild
Location of contractions
Start in the back and spread to the abdomen
Abdomen or groin
Uterine consistency when palpated
Hard as a board; can’t be indented
Easily indented with a finger
Regularity of contractions
Regular with increasing frequency and duration
Irregular; no discernible pattern; tends to decrease in intensity and frequency with activity
Frequency and duration of contractions affected by position or activity
No
Yes
Ruptured membranes
Possible
No
Increased level of activity
After having endured increased fatigue for most of the third trimester, it’s common for a woman to experience a sudden increase in energy before true labor starts. This phenomenon is sometimes referred to as “nesting” because, in many cases, the woman directs this energy toward last-minute activities, such as organizing the baby’s room, cleaning and straightening her home, and preparing other children in the household for the new arrival.
A built-in energy source
The woman’s increase in activity may be caused by a decrease in placental progesterone production (which may also be partly responsible for the onset of labor) that results in an increase in the release of epinephrine. This epinephrine increase gives the woman extra energy for labor.
Braxton Hicks contractions
Braxton Hicks contractions are mild contractions of the uterus that occur throughout pregnancy. They may become extremely strong a few days to a month before labor begins, which may cause some women, especially a primipara, to misinterpret them as true labor. Several characteristics, however, distinguish Braxton Hicks contractions from labor contractions.
Patternless
Braxton Hicks contractions are irregular. There’s no pattern to the length of time between them and they vary widely in their strength. They gradually increase in frequency and intensity throughout the pregnancy, but they maintain an irregular pattern. In addition, Braxton Hicks contractions can be diminished by increasing activity or by eating, drinking, or changing position. Labor contractions can’t be diminished by these activities.
Painless
Braxton Hicks contractions are commonly painless—especially early in pregnancy. Many women feel only a tightening of the abdomen in the first or second trimester. If the woman does feel pain from these contractions, it’s felt only in the abdomen and the groin—usually not in the back. This is a major difference from the contractions of labor.
No softening or stretching
Probably, the most important differentiation between Braxton Hicks contractions and true labor contractions is that Braxton Hicks contractions don’t cause progressive effacement or dilation of the cervix. The uterus can still be indented with a finger during a contraction, which indicates that the contractions aren’t efficient enough for effacement or dilation to occur.
Ripening of the cervix
Ripening of the cervix refers to the process in which the cervix softens to prepare for dilation and effacement. It’s thought to be the result of hormone-mediated biochemical events that initiate breakdown of the collagen in the cervix, thus causing it to soften and become flexible. As the cervix ripens, it also changes position by tipping forward in the vagina.
Ripening of the cervix doesn’t produce outwardly observable signs or symptoms. The ripeness of the cervix is determined during a pelvic examination, usually in the last weeks of the third trimester.
Signs of true labor
Signs of true labor include uterine contractions, bloody show, and spontaneous rupture of membranes.
Uterine contractions
The involuntary uterine contractions of true labor help effacement and dilation of the uterus and push the fetus through the birth canal. Although uterine contractions are irregular when they begin, as labor progresses they become regular with a predictable pattern.
Early contractions occur anywhere from 5 to 30 minutes apart and last about 30 to 45 seconds. The interval between the contractions allows blood flow to resume to the placenta, which supplies oxygen to the fetus and removes waste products. As labor progresses, the contractions increase in frequency, duration, and intensity. During the transition phase of the first stage of labor—when contractions reach their maximum intensity, frequency, and duration— they each last 60 to 90 seconds and recur every 2 to 3 minutes.
Only gold members can continue reading. Log In or Register to continue







 cephalic
cephalic breech
breech shoulder
shoulder compound.
compound.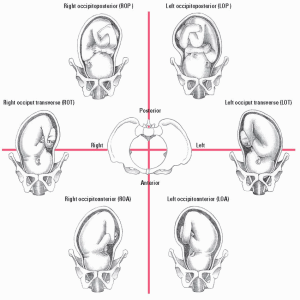



 Advice from the experts
Advice from the experts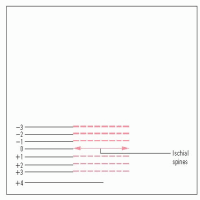

 Advice from the experts
Advice from the experts
 Advice from the experts
Advice from the experts

 Advice from the experts
Advice from the experts




