Intussusception
Considered a pediatric emergency, intussusception occurs when a portion of the bowel telescopes or invaginates into an adjacent bowel portion. (See What happens in intussusception.) This disorder can lead to bowel obstruction and other serious complications. Treatment shouldn’t be delayed.
Intussusception is most common in infants and occurs three times more often in males than in females; approximately 87% of children with intussusception are younger than age 2, and about 70% of these children are between ages 3 months and 12 months.
Causes
In infants, intussusception usually arises from unknown causes. In older children, polyps, hemangioma, lymphosarcoma, lymphoid hyperplasia, Meckel’s diverticulum, or alterations in intestinal motility may trigger the process. In adults, intussusception most commonly results from benign or malignant tumors (65% of patients); other possible causes include polyps, Meckel’s diverticulum, gastroenterostomy with herniation, and an appendiceal stump.
In addition, studies suggest that intussusception may be linked to viral infections because seasonal peaks are observed—in the spring and summer, coinciding with peak incidence of enteritis, and in midwinter, coinciding with peak incidence of respiratory tract infections.
What happens in intussusception
In intussusception, a bowel segment invaginates and is propelled along by peristalsis, pulling in more bowel. In this illustration, a portion of the cecum invaginates and is propelled into the large intestine. Intussusception typically produces edema, hemorrhage from venous engorgement, incarceration, and obstruction.
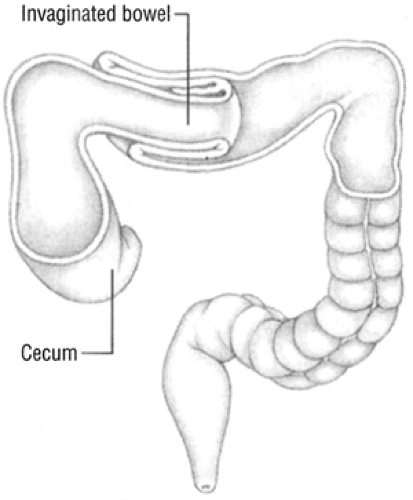 Figure. No caption available |
Complications
Assessment
If the patient is an infant or child, the history may reveal intermittent attacks of colicky pain. Typically, this pain causes the child to scream, draw his legs up to his abdomen, turn pale and diaphoretic, and possibly grunt. Parents may report that the child vomits—initially, stomach contents and, later, bile-stained or fecal material.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


