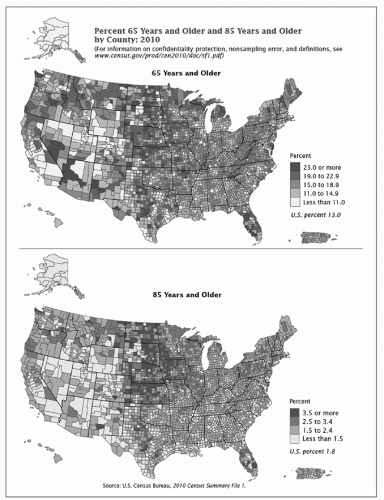
Although people age at different rates, changes to the human body are a hallmark of aging. Normal aging, beyond the effects of disease, is a complex process that involves many different body systems and presents in a wide variety of symptoms and syndromes (Smith & Cotter, 2012). Advances in medical science and technology have resulted in an increased life span. In 2010, older adults comprised approximately 13% of the US population (U.S. Census Bureau, 2011). Along with the growth of the general elderly population has come a remarkable increase in the number of Americans reaching age 100. The segment of the population aged 65 years and older increased most dramatically between 1990 and 2000 by 15.1%. In the same decade, older adults between 85 and 94 years experienced the fastest rate of growth by 29.9% and those over 95 years by 25.9% (U.S. Census Bureau, 2011). By 2030, the older adult population will reach about 72.1 million. Two maps demonstrate the percent of individuals aged 65 years and older and 85 years and older, living in US counties at the time of the 2010 census. This information can be used for planning care requirements for this population and for the numbers of nurses and additional education needed in infusion therapy for the older adult (Figure 22-1).
As the population continues to age, the health care system will need to respond accordingly. Health care professionals will be working with an increasing number of older adults, chronic diseases, and accompanying treatments; the challenges of geriatric syndromes will take on greater importance. Health care professionals’ preparation and competence to care for older adults are of serious concern. Nurses are in a pivotal role to influence the overall quality of care of older adults. Initiatives have been underway for several years to increase the competence of nurses at the point of care to understand the processes of aging and best practices to effectively manage age-related changes as well as the spectrum of diseases and other conditions that often are associated with aging. Physical capacity, the body’s ability to perform various functions, and functionality, the effectiveness of performing activities such as activities of daily living, can both be adversely affected by aging and may require interventions to correct or minimize these effects.
FIGURE 22-1 Individuals (in percentage) aged 65 years and older (top) and 85 years and older (bottom) by US county in 2010. (From U.S. Census Bureau. (2011). The older population: 2010-2010 Census Briefs. http://www.census.gov/prod/cen2010/briefs/c2010br-09.pdf)
Infusion therapy is one method of delivering various treatments that can be very effective for the older adult. However, there are special considerations that must be taken into account for this therapy to have quality outcomes. This chapter addresses the important considerations in initiating, delivering, and maintaining infusion therapy in the older adult patient. The term older adult describes a broad category of individuals who range from 50 to 100 years of age, though the term is generally associated with individuals aged 65 years and older. Many physiologic changes associated with the older adult begin in the sixth decade of life, although variations exist among individuals. Infusion nurses caring for older adults are supported in the need for additional clinical knowledge and technical expertise with the Infusion Nurses Society (INS) (2011) standard on older adult patients (p. S7-S8). The document is a guide to the needs of the older adult patient and organizational resources.
THE OLDER ADULT PATIENT AS A HEALTH CARE CONSUMER
As a consumer of health care, the older adult patient has special needs associated with the aging process that challenge the health care system and health care providers. The older adult patient may require administration of complex infusion therapies to treat a multitude of clinical conditions that may occur simultaneously. Older adults today are educated consumers. For some, adopting healthy lifestyles, such as engaging in regular physical activity and eating a healthy diet has reduced the risk of chronic disease as well as the rate of disability. These same lifestyle behaviors also help older adults better manage their chronic diseases. In the past, patients did not usually question the wisdom of their provider, and took a more passive approach to decision-making. Today, issues of informed consent and self-determination have become more prominent, and most patients, young and older adults alike, are taking a much more active role in planning treatments that are effective and personally acceptable. Many older patients are collaborating with their providers and partnering with them to monitor the decisions that they, as consumers, make. Decisions that are clinically relevant and ethically appropriate are the challenges of the caregiver and older adult; there must be a careful balance of such in light of medical requirements and what resources will be beneficial and available (Mitty & Post, 2012).
EVIDENCE FOR PRACTICE
In 2011, the cost of chronic disease totaled nearly $3 trillion. What will the impact of chronic disease be in the future? How will self-management affect the financial burden?
Physiology of Aging: Homeostasis
The kidneys, heart and blood vessels, lungs, skin, adrenal glands, hypothalamus, pituitary gland, parathyroid gland, and gastrointestinal tract are the regulatory organs associated with maintaining the body’s homeostasis. Homeostasis is the ability of the body to maintain a balance of volume and composition of body fluids within normal ranges. The kidneys are a primary force in homeostasis because they work to adjust the amount of water and electrolytes that exit the body in an amount equal to the quantity of solution entering the body, through either parenteral or oral feedings. Circulating blood reaches the kidneys in sufficient volume to regulate water and electrolytes, and the pumping action of the heart provides circulation through the kidneys, which produce and excrete urine.
The lungs are involved in homeostasis through ventilation. Antidiuretic hormone (ADH), which causes fluid retention, is manufactured in the hypothalamus and stored in the pituitary gland. ADH also is involved in controlling blood volume. When blood volume is increased, ADH secretion is decreased and water is excreted through the kidneys. Parathyroid hormone affects calcium and phosphate concentrations and influences reabsorption of calcium, a key factor in maintaining fluid and electrolyte monitoring and replacement. The gastrointestinal tract also plays a major role in homeostasis by absorption and reabsorption through the small intestine. For the body to maintain homeostasis, all these organs must work in synchronicity.
In otherwise healthy adults, physiologic changes may cause reactions related to medication changes—that is, they influence the absorption, distribution, and clearance of medications. Absorption in older adults is complete, yet slower. Age-related changes also affect the rate and extent of absorption. As people age, they lose lean body mass and gain adipose tissue. With less fluid available, water-soluble medications can reach toxic levels more quickly. Vigilant monitoring is needed with potentially nephrotoxic agents, H2-antagonists, hypoglycemics, and nonsteroidal anti-inflammatory agents. With decreases in kidney and liver function, clearance and excretion of drugs also take longer. Monitoring serum protein and albumin levels, as well as renal and liver functions, is essential to help the older patient avoid toxicity or undertreatment (Amella, 2004).
Normal homeostatic mechanisms in aging become less efficient in the face of external trauma, surgical intervention, disease process, or infection. The older patient is vulnerable to complications associated with routine infusion therapy. An overview of age-related physiologic changes is summarized in Table 22-1.
Physiology of Aging: The Immune System
With aging, the immune system undergoes natural changes and declines. There is a reduced efficiency of the immune response, both from the innate immune system, which is responsible for an immediate response to bacteria or viruses, and the adaptive immune system, which elicits a delayed response and is often more effective once activated (Graham, Christian, & Kiecolt-Glaser, 2006). Because of this natural decrease in function, older adults are at greater risk for impairment and death from infection. They are especially at risk for intravenous catheter-associated infection due to their potentially immunocompromised status.
Physiology of Aging: The Cardiovascular System
Cardiovascular changes are profound, contributing to a slower response to the stress of blood loss, fluid depletion, shock, and acid-base imbalances. Changes in renal and cardiac status have the potential to place the patient at great risk for the development of infusionrelated complications.
TABLE 22-1 THE AGING OF THE BODY’S SYSTEMS
Body System
Physiologic Changes
Signs/Symptoms
Skin
Loss of subcutaneous tissue and thinning of the dermis
Underlying tissue more fragile; inability to respond to heat or cold quickly; proneness to heat stroke; loss of moisture; wrinkling
Sensory
Loss of lid elasticity
Ocular changes in the cornea, iris, pupil, lens
Eyelids droop or turn inward
Increased astigmatism; need for more light; glare problems; need for eyeglasses
Cataracts
Auditory canal narrows
Calcification of ossicles
Changes in the organ of Corti
Olfactory bulb and cells decrease
Increased cerumen
Hearing loss
Impaired sound transmission; tinnitus
Inability to discriminate odors
Cardiovascular
Decreased stress response
Stiffer valves
Conductivity altered
Diminished cardiac output
Diastolic murmurs
More ectopic beats; less ability to respond to changes in blood pressure
Vessels less elastic
Poorer perfusion to vital organs with resulting hypoxia; varicosities; peripheral pulses not always palpable
Pulmonary
Enlargement and rigidity of the chest wall
Airway collapse
Poor expansion with less efficient air exchange; shallow breathing; less effective cough
Less efficient oxygen exchange
Gastrointestinal
Increase in incidence of hiatal hernia
Decrease in abdominal strength
Reduced gastric acid
Slowed neural transmission
Weakened intestinal walls
Reflux
Peptic ulcers
Vitamin deficiencies
Constipation
Incontinence
Diverticulosis
Renal
Decrease in renal blood flow, and glomerular filteration rate
Decreased creatinine clearance
Decreased ability to concentrate urine and conserve water
Poor response to stress
Musculoskeletal
Shrinkage of vertebral discs
Loss of bone mass
Muscle atrophy
Loss of height by 1.5-3 inches
Tendency toward fractures
Decreased strength
Decreased stamina
Neurologic
Diminished REM sleep
Altered pain sensation
Tactile sense decreases
Sleep disorders
Difficulty with balance and position changes
Decreased perception of pain
Loss of sensation in the extremities
Immune
Decrease in thymus mass
Increase in immunoglobulins
Decline in cell-mediated immunity with possible reactivation of herpes, tuberculosis
Autoimmune response not associated with disease
Endocrine
Loss of sensitivity to insulin
Decrease in sex hormones
Blood glucose does not return to normal as rapidly
BPH, testicular firmness; vaginal dryness and atrophy
Longer time to orgasm
BPH, benign prostatic hypertrophy; REM, random eye movement.
Adapted from Jett, K. (2012). Chapter 4: Physiological changes. In T. A. Touhy & K. Jett, Ebersole & Hess’ Toward healthy aging: Human needs & nursing response (8th ed., pp. 44-61). St. Louis, MO: Elsevier/Mosby.
PATIENT SAFETY
Fluid volume excess or hypervolemia, also called fluid overload, is a serious risk in the older adult patient receiving IV fluids. Using an electronic infusion device, monitoring lung sounds, and dividing blood components into smaller amounts, or aliquots, are recommended practices especially for older adult patients.
Physiology of Aging: Skin and Connective Tissue
The skin, the body’s first defense against disease, changes in texture, depth, and integrity as the person ages. After age 60, epidermal cell replacement decreases, resulting in a marked thinning of the epidermis and an increased fragility of the skin’s surface. The result is dry, transparent, paper-thin tissue that tears easily and heals slowly. Changes in the dermis create a loose, wrinkling effect. The skin becomes pale, and nerve endings are less sensitive. The older adult is at risk for thermal injuries. Subcutaneous fat cells decrease, resulting in changes to the superficial fascia, including decreased production of sebum and sweat. Loss of subcutaneous tissue and resultant thinning of the skin present a venous access challenge. Purpura and ecchymoses may appear because of dermal fragility; minor trauma may inflict bruising.
PATIENT SAFETY
Because of fragile skin and less tissue support, stroking the veins gently to promote venous filling is recommended rather than patting, which may cause bruising and tissue damage.
Physiology of Aging: Fluid Balance
Physiologic changes of aging affect the older adult’s fluid balance. Fluid reserves are limited, and total body water is reduced by 6%, creating a potential for fluid volume deficit. Gastrointestinal changes such as decreased volume of saliva and gastric juice and decreased calcium absorption cause the mouth to be drier and increase potential for sodium and potassium deficit during episodes of vomiting and gastric suction. Oral intake may be altered as a result of medications, treatments, advanced cognitive impairment, swallowing impairments, and other functional challenges (Gilmour & Penny, 1991). Assessment guidelines are presented in Box 22-1.
Only gold members can continue reading. Log In or Register to continue
 EVIDENCE FOR PRACTICE
EVIDENCE FOR PRACTICE PATIENT SAFETY
PATIENT SAFETY PATIENT SAFETY
PATIENT SAFETY


