Heart Valve Replacement
Severe valvular stenosis or insufficiency commonly requires excision of the affected
valve and replacement with a mechanical or biological prosthesis. The mitral and aortic valves are most commonly affected because of the high pressure generated by the left ventricle during contraction.
valve and replacement with a mechanical or biological prosthesis. The mitral and aortic valves are most commonly affected because of the high pressure generated by the left ventricle during contraction.
Comparing prosthetic valves
Both mechanical and bioprosthetic valves are commonly used. A mechanical valve, such as a leaflet valve, can withstand considerable stress. Because this type of valve tends to last longer than bioprosthetic valves, it’s usually implanted in younger patients to avoid the need for another operation in the future. Because blood flow is turbulent through the valve, the patient usually requires long-term anticoagulant therapy to prevent thrombus formation.
Bileaflet valve
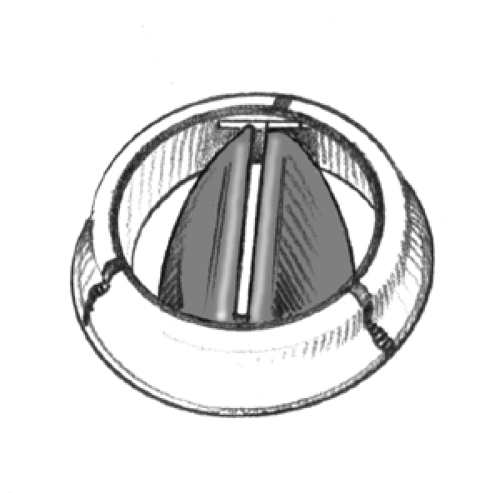 Figure. No caption available |
The bioprosthetic heart valve, such as a porcine or bovine valve, doesn’t obstruct blood flow as much as a mechanical valve and is less likely to cause thrombus formation. In addition, a bioprosthetic valve doesn’t require prolonged anticoagulant therapy. However, the valve is difficult to insert and less durable (prone to degeneration or calcification, especially in patients with renal disease) than its mechanical counterpart. Despite these drawbacks, the physician will probably select a biological prosthetic valve for implantation if the patient appears unlikely to comply with anticoagulant therapy.
Porcine valve
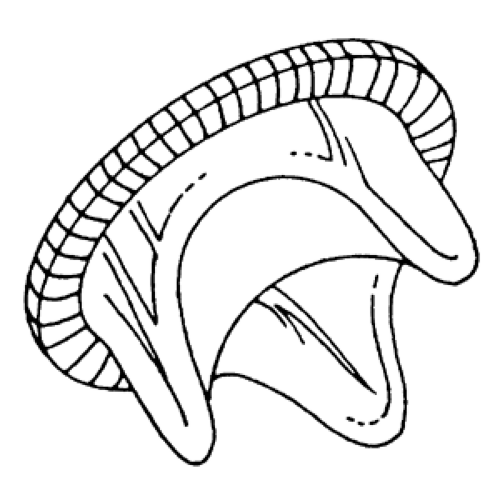 Figure. No caption available |
Indications for valve replacement depend on the patient’s symptoms and the affected valve. For example, if the patient has severe symptoms that can’t be managed with drugs and dietary restrictions, a commissurotomy may be performed. If this isn’t successful, valve replacement may be done. In aortic insufficiency, valve replacement is usually done when symptoms—palpitations, dizziness, dyspnea on exertion, angina, and murmurs—have developed or if the chest X-ray and electrocardiogram (ECG) reveal left ventricular hypertrophy. In aortic stenosis, which may be asymptomatic, valve replacement may be performed if cardiac catheterization reveals significant stenosis. In mitral stenosis, it’s indicated if the patient develops fatigue, dyspnea, hemoptysis, arrhythmias, pulmonary hypertension, or right ventricular hypertrophy. In mitral insufficiency, surgery is usually done when the patient’s symptoms—dyspnea, fatigue, and palpitations—interfere with his activities or if insufficiency is acute, as in papillary muscle rupture.
Diseased or damaged mitral or aortic valves may be replaced by either mechanical or bioprosthetic heart valves. (See Comparing prosthetic valves.)
Procedure
After performing a medial sternotomy and initiating cardiopulmonary bypass, the surgeon cannulates the coronary arteries and perfuses them with a cold cardioplegic solution. For aortic valve replacement, he clamps the aorta above the right coronary artery; for mitral valve replacement, he incises the left atrium to expose the mitral valve.
After excising the diseased valve, the surgeon sutures around the margin of the valve annulus (the ring or encircling structure, which is left intact after valve excision). He then threads the suture material through the sewing ring of the prosthetic valve and, using a valve holder,




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
