Many obstetric complications involve the possibility of hemorrhage, requiring blood replacement. Determine the patient’s feelings and beliefs regarding the possibility of transfusions, and notify health care providers if transfusion is refused.
Ectopic Pregnancy
Ectopic pregnancy is a gestation that implants outside the uterine cavity. Locations typically include the fallopian tube (96%), ovary, cervix, or abdominal cavity (Figure 39-1). Most tubal pregnancies occur in the distal (ampullary) two thirds of the tube. Some are located in the proximal portion of the extrauterine part of the tube (isthmic).
Etiology
Clinical or structural factors that prevent or delay the passage of the fertilized ovum:
Pelvic inflammatory disease.
Prior history of ectopic pregnancy.
Prior tubal surgery or curettage.
Diethylstilbestrol (DES) exposure.
Adhesions or infections of the tube; salpingitis.
Congenital and developmental anomalies of the fallopian tube or uterus.
Increased maternal age.
Elective reversed sterilizations.
The growing ectopic pregnancy may result in inflammation, rupture, hemorrhage, peritonitis, or death.
Clinical Manifestations
Abdominal or pelvic pain (typically unilateral).
Irregular vaginal bleeding—usually scanty and dark (most common).
Amenorrhea—75% of the cases.
Uterine enlargement: size equates to normally implanted pregnancy.
Abdominal tenderness on palpation.
Radiating shoulder pain (due to bleeding aggravating nerves in the peritoneal cavity).
Increased pulse and anxiety.
Nausea, vomiting, faintness, vertigo, or syncope.
Pelvic examination may reveal a pelvic mass, posterior or lateral to the uterus, adnexal tenderness, and cervical pain with movement of the cervix.
Figure 39-1. Sites of ectopic pregnancy.
NURSING ALERT
Pain may become severe if the fallopian tube ruptures; clinical presentation will evolve into shock acutely or chronically.
Diagnostic Evaluation
Serial quantitative levels of the beta subunit of human chorionic gonadotropin (β-hCG) can be used in combination with ultrasound in most cases to confirm diagnosis.
Serum β-hCG (produced by trophoblastic cells)—serial evaluations will not show characteristic rise as in intrauterine pregnancy.
Transvaginal ultrasound—identifies tubal mass and absence of gestational sac within the uterus.
Serum progesterone—reflects production of progesterone by the corpus luteum stimulated by a viable pregnancy; 97.5% sensitivity if serum progesterone levels are greater than or equal to 25 ng/mL (greater than or equal to 79.5 nmol/L), signifying further testing is warranted.
Culdocentesis—bloody aspirate from the Cul-de-sac of Douglas, the posterior fornix of the vagina, indicates intraperitoneal bleeding from tubal rupture.
Laparoscopy—abdominal visualization of tubal pregnancy (considered the diagnostic gold standard).
Laparotomy—indication for surgery if there is any question about the diagnosis.
Management
Conservative Therapy
Conservative therapy is chosen should the patient desire future childbearing and clinical conditions stable. Methotrexate is considered first-line treatment, if applicable: hemodynamically stable without active bleeding or signs of hemoperitoneum, or general anesthesia poses a risk, or patient is unable to return for follow-up care. Contraindications to methotrexate include breastfeeding, immunodeficiency, alcoholism, liver disease, pulmonary disease, peptic ulcer disease, renal dysfunction, or blood dyscrasias.
Methotrexate dosing:
Single-dose methotrexate (50 mg/m2) I.M.
Multiple-dose methotrexate (1 mg/kg) I.M. every other day (days 1, 3, etc.), accompanied with leucovorin (0.1 mg/kg) I.M. every other day (days 2, 4, 6, etc.). Regimen is followed until the β-hCG drops 15% or more in 48 hours or four doses of methotrexate have been given.
Goal of treatment is to remove ectopic pregnancy and preserve tubal patency as well as reproductive function.
Surgical Treatment
If woman does not consent to or meet criteria for methotrexate, surgical intervention is instituted. The surgical procedure depends on the extent of tubal involvement and if rupture has occurred.
The surgery of choice used to preserve future fertility is a salpingostomy (removes conceptus leaving tube intact, yet scarred).
Should a woman not desire future fertility, the surgery of choice is salpingectomy (removal of portion of fallopian tube with conceptus).
Other surgeries range from removal of ectopic pregnancy with tubal resection, salpingostomy, and possibly salpingo-oophorectomy (removal of tube and ovary on affected side).
Treat shock and hemorrhage accordingly as clinical conditions warrant.
Administer RhIG (immune globulin) per facility’s policy if woman is Rh negative.
Complications
Infertility.
Hemorrhage and death.
Nursing Assessment
Evaluate the following to determine pregnancy status and to monitor for clinical changes in patient, such as ectopic rupture or hemorrhage:
Maternal vital signs.
Presence and amount of vaginal bleeding.
Amount, type, and evolving intensity of pain.
Presence of abdominal tenderness on palpation accompanied by radiating shoulder pain.
Date of last menses.
Presence of positive pregnancy test.
Rh type.
Nursing Diagnoses
Deficient Fluid Volume relative to blood loss from ruptured fallopian tube.
Acute Pain related to ectopic pregnancy or rupture and bleeding into the peritoneal cavity.
Anticipatory Grieving related to loss of pregnancy and potential loss of childbearing capacity.
Nursing Interventions
Maintaining Fluid Volume
Establish an intravenous (IV) line with a large-bore catheter (#16 to #18G) and infuse fluids; blood component therapy may be prescribed.
Obtain blood samples for complete blood count (CBC) and type and screen, as directed.
Monitor vital signs and urine output as the patient’s condition warrants.
Promoting Comfort
Administer analgesics, as needed and prescribed.
Encourage the use of relaxation techniques.
Providing Support through the Grieving Process
Be available to patient and provide emotional support; listen to concerns of patient and significant others.
Be aware that patient/family may be experiencing denial or other stages of grief; grief counseling may be appropriate.
Note: The term family may refer to a nontraditional group of persons, such as the patient and significant other, friend, sibling, parent, or grandparent.
Patient Education and Health Maintenance
Teach signs and symptoms of ectopic pregnancy to women at risk: increased vaginal bleeding, moderate to severe abdominal pain (typically unilateral and low), shoulder pain, nausea, and vomiting.
Instruct woman to report relative signs and symptoms to primary practitioner or emergency department immediately.
Encourage grief counseling and supportive care at home.
Discuss contraception.
Evaluation: Expected Outcomes
Vital signs stable.
Verbalizes pain relief.
Patient and support person express appropriate grief response.
Gestational Trophoblastic Disease
Gestational trophoblastic disease (“molar pregnancy”) comprises myriad interrelated conditions, originating from anomalous development of the placenta. It is characterized by the conversion of the chorionic villi into a mass of clear vesicles. There may be no fetus or a degenerating fetus may be present. The diagnosis may include complete and partial hydatidiform moles, invasive moles, gestational choriocarcinomas, and placental site trophoblastic tumors. The rate of occurrence is 1:1,500 pregnancies or 1:600 therapeutic abortions. Molar pregnancies are usually diagnosed during the first trimester of pregnancy and may require chemotherapy.
Pathophysiology and Etiology
Features of a partial or complete hydatidiform mole include the following abnormalities:
Karyotype—derived from genetic abnormalities as the paternal haploid, X-carrying set of chromosomes that reaches 46, XX (or 46, XY) by its own duplication in a complete mole and 69, XXX (or 69, XXY) in a partial mole.
Pathology—fetus may or may not be present, amnion and fetal red blood cells (RBCs) may be present, villous edema may be focal or diffuse throughout (complete); trophoblastic proliferation may be slight to severe.
Clinical Manifestations
First-trimester vaginal bleeding.
Absence of fetal heart tones and fetal structures.
Uterine enlargement greater than dates (size may double if complete mole exists).
β-hCG titers greater than expected for gestational age.
Expulsion of the vesicles.
Hyperemesis gravidarum (severe nausea and vomiting).
Early onset of preeclampsia; first half of pregnancy.
Diagnostic Evaluation
β-hCG levels—excessive elevations.
Ultrasound—diffuse mixed echogenic pattern replacing the placenta (clear “grapelike” structures fill the uterine cavity accompanied by absent fetus or partial development).
Management
Approximately 20% of patients will develop malignant sequelae, requiring administration of chemotherapy after evacuation of hydatidiform moles.
Suction curettage is the method of choice for immediate evacuation of the mole with possibility of laparotomy; hysterectomy may be an option but rare.
Serial quantitative β-hCG determinations should be performed to confirm resolution to baseline values (<5 mIU/mL). Persistent elevations indicate malignant postmolar gestational trophoblastic disease.
Hormonal contraception during β-hCG monitoring.
Chemotherapy for patients with malignant gestational trophoblastic disease.
Administer RhIG per your facility’s policy if woman is Rh negative.
Complications
Significant blood loss.
Malignancy.
Infertility.
Nursing Assessment
Monitor vital signs; note symptoms of early-onset preeclampsia (discussed later in chapter).
Assess the amount and type of vaginal bleeding; note the presence of other vaginal discharge.
Assess for proteinuria (elevated levels of protein in urine).
Determine date of last menstrual period (LMP) and date of positive pregnancy test.
Measure fundal height, via tape or palpation, and compare to LMP.
Evaluate CBC results and Rh type.
Nursing Diagnoses
Risk for deficient Fluid Volume related to maternal hemorrhage.
Anxiety related to loss of pregnancy and medical interventions.
Nursing Interventions
Maintaining Fluid Volume
Obtain blood samples for type and screen; blood component therapy may be indicated, prepare accordingly.
Establish and maintain peripheral IV line; start with a large needle (#16 to #18G) to accommodate anticipatory need for transfusion and/or large quantities of fluid.
Assess maternal vital signs and evaluate bleeding as patient’s condition warrants.
Monitor laboratory results to evaluate patient’s status.
Decreasing Anxiety
Prepare the patient for surgery. Explain preoperative and postoperative care along with intraoperative procedures.
Educate patient and family on the disease process—acute and chronic aspects.
Allow the family to grieve over the loss of pregnancy and possible infertility.
Patient Education and Health Maintenance
Advise the woman on the importance of continuous followup care.
Provide reinforcement of follow-up procedures; typically lasts up until 1 year postdiagnosis.
Encourage ongoing discussion of care and fertility options with health care provider.
Evaluation: Expected Outcomes
Vital signs stable; laboratory work within normal limits.
Verbalizes concerns about self and related procedures; describes follow-up care and its importance.
Spontaneous Abortion
Evidence Base
American College of Obstetricians and Gynecologists. (2005/Reaffirmed 2011). Medical management of abortion (Practice Bulletin #67). Washington, DC: Author.
Spontaneous abortion occurs as a natural termination of pregnancy prior to 20 weeks. Variations are outlined in Table 39-1. Medical termination of a pregnancy is known as a therapeutic (maternal or fetal indications) or voluntary abortion, accomplished through medication administration or surgical intervention.
Pathophysiology and Etiology
Natural causes commonly unknown, yet 50% are due to chromosomal anomalies.
Exposure or contact with teratogenic agents.
Poor maternal nutritional status.
Maternal illness with virus, such as rubella, cytomegalovirus, active herpes, and toxoplasmosis, or specific bacterial microorganisms that put the pregnancy at risk.
History of diabetes, thyroid disease, anticardiolipin antibodies, or lupus erythematosus.
Smoking, illicit drug abuse, or both.
Immunologic or genetic factors.
Luteal phase defect.
Abnormal or postmature sperm or ova.
Abnormal uterine development or structural defect in the maternal reproductive system (including an incompetent cervix).
Presence of intrauterine device.
Environmental factors such as chemicals, radiation, or trauma.
Clinical Manifestations
Uterine cramping, lower back pain.
Vaginal bleeding usually begins as dark spotting, then progresses to frank bleeding.
hCG levels may be elevated for as long as 2 weeks after loss of embryo.
Diagnostic Evaluation
Ultrasonic evaluation of the gestational sac or embryo.
Visualization of the cervix; presence of dilation or tissue expulsion.
Complications
Hemorrhage.
Uterine infection.
Septicemia may occur due to missed/undiagnosed abortion.
Disseminated intravascular coagulation (DIC) rare but may occur with a missed abortion.
Nursing Assessment
Determine date of LMP and date of positive pregnancy test.
Monitor maternal vital signs: assess for hemorrhage or infection.
Evaluate blood loss: initiation, duration, estimated total amount, precipitating factors.
Evaluate any blood or clot tissue for the presence of amniotic membranes, placenta, or fetus.
Table 39-1 Types of Spontaneous Abortions
CLASSIFICATION
CLINICAL MANIFESTATIONS
MANAGEMENT
Threatened
Vaginal bleeding or spotting
Mild cramps
Tenderness over uterus, simulates mild labor or persistent lower backache with feeling of pelvic pressure
Cervix closed or slightly dilated
Symptoms subside or develop into inevitable abortion
Vaginal examination
Bed rest (some clinicians will not limit activity in belief that the embryo will be aborted anyway)
Pad count
Inevitable
Bleeding more profuse
Cervix dilated
Membranes rupture
Painful uterine contractions
Embryo delivered, followed by dilatation and evacuation (D&E)
Habitual
Spontaneous abortion occurs in successive pregnancies (three or more)
D&E
Treatment of possible causes: hormonal imbalance, tumors, thyroid dysfunction, abnormal uterus, incompetent cervix; with treatment, 70% to 80% carry a pregnancy successfully
Hysterogram to rule out uterine abnormalities, infections
Surgical suturing of the cervix if incompetent cervix is a causative factor
Incomplete
Fetus usually expelled
Placenta and membranes retained
D&E
Missed
Fetus dies in utero and is retained
Maceration
No symptoms of abortion, but symptoms of pregnancy regress (uterine size, breast changes)
Real-time ultrasound, and if second trimester, fetal monitoring to determine if fetus has died
D&E if early pregnancy
If fetus is not passed after diagnosis, oxytocin induction may be used; retained dead fetus may lead to development of disseminated intravascular coagulation or infection
Fibrinogen concentrations should be measured weekly
Nursing Diagnoses
Risk for Deficient Fluid Volume related to maternal bleeding.
Anticipatory Grieving related to loss of pregnancy, cause of the abortion, future childbearing.
Risk for Infection related to dilated cervix and open uterine vessels.
Acute Pain related to uterine cramping and possible procedures.
Nursing Interventions
Maintaining Fluid Volume
Draw blood for CBC as well as type and screen, as directed, to assess blood loss and prepare for transfusion.
Assess and report to the perinatal team signs of hemorrhage: tachycardia, hypotension, hyperventilation, altered level of consciousness (LOC), diaphoresis, or pallor.
Establish and maintain an IV line with large-bore catheter (#16 to #18G) for possible transfusion and large quantities of fluid replacement; two IV lines may be warranted.
Inspect all expelled tissue and assess for completeness; retained products of conception may lead to further bleeding and, possibly, hemorrhage if not completely expelled.
Providing Support through the Grieving Process
Evaluate need for grievance counseling; offer support.
Do not minimize the loss by focusing on future childbearing; rather, acknowledge the loss and allow grieving. Every pregnancy, irrelevant to the length of gestation, deserves recognition and respect of acknowledgment.
Provide time alone for the couple to discuss their feelings and to grieve.
Discuss the prognosis of future pregnancies with the patient and support persons.
Provide an opportunity for viewing the fetus per patient request.
Refer to chaplain or social worker, if indicated or requested.
Preventing Infection
Evaluate temperature and pulse for signs of infection periodically.
Assess vaginal drainage for increased amount and odor; may indicate infection.
Educate and encourage perineal care after each urination and defecation to prevent contamination.
Promoting Comfort
Instruct patient on the cause of pain to decrease anxiety.
Instruct and encourage the use of relaxation techniques to augment analgesics.
Administer pain medications, as needed and prescribed.
Community and Home Care Considerations
Review symptoms of hemorrhage if a threatened abortion is suspected.
Discuss an emergency access care plan with patient and support personnel.
Instruct the patient to collect any expelled specimen and to bring to facility with her for evaluation.
Patient Education and Health Maintenance
Provide the names of local support groups; Resolve Through Sharing groups may be available through a local hospital.
Discuss with the patient methods of contraception to be used.
Explain the need to wait 2 to 4 months before attempting another pregnancy.
Teach the woman to observe for signs of infection (fever, pelvic pain, change in character and amount of vaginal discharge) and advise to report to provider immediately.
Provide information regarding genetic testing of the products of conception, if indicated; send the specimen according to facility policy.
Evaluation: Expected Outcomes
Vital signs remain normal; minimal blood loss.
Expresses feelings regarding the loss of the pregnancy by demonstrating normal signs of grief.
No signs of infection, temperature normal, performs perineal care.
Verbalizes relief of pain.
Hyperemesis Gravidarum
Evidence Base
American College of Obstetricians and Gynecologists. (2004/Reaffirmed 2011). Nausea and vomiting in pregnancy (Practice Bulletin #52). Washington, DC: Author.
Hyperemesis gravidarum is exaggerated and persistent nausea and vomiting that occurs during pregnancy. It is a clinical diagnosis of exclusion based on a typical presentation in the absence of other diseases that could explain the findings, such as GI conditions, metabolic disease, neurologic disorders, drug use, or acute fatty liver or preeclampsia during pregnancy.
Pathophysiology and Etiology
Typically occurs during the first 16 weeks’ gestation but may last into the third trimester in severe cases. Etiology is unknown, but two theories prevail: psychosomatic or hormonal stimulus (high levels of β-hCG or estrogen).
Accompanied by appetite disturbances that are intractable in nature.
Psychological factors, including neurosis or altered self-concept, may be contributory.
Seen in molar pregnancies, multiple gestation, and history of hyperemesis in previous pregnancies.
Decreased gastric motility often accompanies the condition.
Persistent vomiting may result in fluid and electrolyte imbalances, dehydration, jaundice, and elevation of serum transaminase.
Clinical Manifestations
Persistent vomiting; inability to tolerate anything by mouth.
Dehydration—fever, dry skin, decreased urine output, large ketonuria.
Weight loss (up to 5% to 10% of body weight).
Severity of symptoms commonly increases as the condition progresses.
Diagnostic Evaluation
Tests may be done to rule out other conditions causing vomiting (cholecystitis, appendicitis, pancreatitis, thyroid disease, or hepatitis).
Liver function studies—alanine aminotransferase (ALT) and aspartate transaminase (AST) are elevated four times normal in severe cases.
Prothrombin time (PT), partial thromboplastin time (PTT) usually normal.
Blood urea nitrogen (BUN) and creatinine—may be slightly elevated.
Serum electrolytes—may result in hypokalemia, hyponatremia, or hypernatremia; loss of hydrogen and chloride.
Ketones in blood and urine.
Management
Try withholding food and fluid for 24 to 48 hours or until vomiting stops and appetite returns; then restart small meals.
Control of vomiting may require anti-emetics (benefits to therapy may outweigh the risks of drugs), such as:
Phenothiazines—prochlorperazine (injectable or rectal suppository); promethazine; or chlorpromazine.
Droperidol.
Metoclopramide—do not give in combination with phenothiazines.
Meclizine.
Methylprednisolone (recently found to be more helpful than promethazine; 16 mg three times per day for 3 days then tapered over 2 weeks).
Treat dehydration with IV fluids—typically 1 to 3 L of dextrose solution with electrolytes and vitamins, as needed.
Most women respond quickly to restricting oral intake and giving IV fluids, but repeated episodes may occur.
Total parenteral nutrition rarely needed.
Complications of hepatic or renal failure or coma could result from disease progression but rare.
Complications
Hypovolemia and renal insufficiency.
Electrolyte imbalance.
Malnutrition.
Nursing Assessment
Evaluate weight loss pattern; compare to prepregnant weight.
Evaluate 24- or 48-hour dietary recall.
Evaluate environmental factors that may affect the woman’s appetite. Determine if woman is ingesting nonfood substances (pica), such as starch, clay, or toothpaste.
Monitor vital signs for tachycardia, hypotension, and fever due to dehydration.
Assess skin turgor and mucous membranes for signs of dehydration.
Nursing Diagnoses
Risk for Deficient Fluid Volume related to prolonged vomiting.
Imbalanced Nutrition: Less Than Body Requirements related to prolonged vomiting.
Ineffective Coping related to stress of pregnancy and illness.
Fear related to concerns for fetal well-being.
Nursing Interventions
Maintaining Fluid Volume
Establish an IV line and administer IV fluids, as prescribed.
Monitor serum electrolytes and report abnormalities.
Medicate with anti-emetics, as prescribed.
Maintain nothing-by-mouth status until vomiting has stopped; introduce ice chips slowly and add clear fluids once tolerated; solid food introduced later.
Assess intake and output, urine specific gravity and ketones, vital signs, skin turgor, and fetal heart rate (FHR), as indicated by condition.
Encouraging Adequate Nutrition
Advise the woman that oral intake can be restarted once emesis ceases and appetite returns.
Begin small bland meals (ie, rice and chicken). Avoid greasy, gassy, and spicy foods.
Suggest or provide an environment conducive to eating.
Administer parenteral calorie replacement if multiple antiemetic treatments and enteral tube feeding have been unsuccessful.
Consult with a dietitian, as indicated.
Strengthening Coping Mechanisms
Allow patient to verbalize feelings regarding this pregnancy and associated stressors.
Refer the patient to social service and counseling services, as needed.
Allaying Fears
Explain the effects of all medications and procedures on maternal as well as fetal health.
Once confirmed, accentuate the positive signs of fetal wellbeing.
Praise and support patient for attempts at following nutritious diet and healthy lifestyle.
Patient Education and Health Maintenance
Educate the woman about proper diet, nutrition, and healthy weight gain.
Educate the woman on the need to take anti-emetics continuously during the nausea phase to alleviate vomiting episodes.
Evaluation: Expected Outcomes
Demonstrates signs of normal hydration with no ketosis; urine output adequate; urine-specific gravity within normal limits; blood pressure (BP) stable.
Tolerates clear liquids then small, bland diet without vomiting.
Verbalizes concerns and stresses related to pregnancy.
Expresses confidence in fetal well-being.
Placenta Previa
Placenta previa is the abnormal implantation of the placenta in the lower uterine segment, partially or completely covering the internal cervical os (Figure 39-2). Classification may change over the course of the pregnancy or during labor as the cervix dilates. Placenta previa occurs in 1 in 200 live births and is associated with intrauterine growth restriction (IUGR).
Figure 39-2. Degrees of placenta previa. (A) Low implantation. (B) Partial placenta previa. (C) Total placenta previa.
Pathophysiology and Etiology
Classifications of placenta previa:
Complete: placenta covers the cervical os completely.
Partial: placenta partially covers the cervical os.
Marginal: placenta lies at the margin of the internal os, but does not cover it.
Low-lying placenta: placental implantation in the lower uterine segment next to the cervical os; the placenta may migrate and be pulled upward as the uterus stretches and grows during the course of the pregnancy.
Causation is unknown, but risk factors include:
Previous myomectomy.
Endometritis.
Scarred uterus to include vaginal birth after cesarean delivery (VBAC).
Induced or spontaneous abortions involving suction curettage.
Cardinal sign is sudden onset of painless vaginal bleeding during the second or third trimester; some women may not exhibit bleeding until labor starts.
Initial episode is rarely fatal and usually stops spontaneously.
With a complete placenta previa, bleeding typically occurs earlier in the pregnancy.
Diagnostic Evaluation
Ultrasound (transabdominal, transvaginal, or translabial) is the method of choice to show location of placental implantation.
Management
Conservative management is usually possible with nonviable pregnancy and maternal stability.
Once viable and fetal lung maturity is established, delivery may be attempted based on maternal-fetal status.
If bleeding is heavy, IV access should be established immediately, along with CBC, type, and crossmatching for blood component therapy, as indicated.
Typically in the medical facility setting, continuous maternal and fetal monitoring is necessary.
Cesarean delivery is usually indicated if maternal-fetal status unstable or complete previa.
Vaginal delivery may be attempted in a marginal or low-lying placenta without active bleeding. Operating room personnel should be available.
Notify neonatal team.
Complications
Placenta accreta (abnormally adherent placenta difficult to expel); increased incidence if placenta previa exists with maternal history of uterine surgery.
Immediate hemorrhage, possible shock, and maternal death.
Postpartum hemorrhage.
Prematurity.
Nursing Assessment
Estimate current episode of blood loss; review history of bleeding throughout current pregnancy.
Assess pain in association with the bleeding.
Assess maternal and fetal vital signs through electronic fetal monitoring (EFM).
Assess for symptoms of labor: preterm or term.
Evaluate laboratory data to assess signs of hemorrhage: hemoglobin and hematocrit.
NURSING ALERT
Withhold vaginal examinations in patients with active vaginal bleeding until placenta previa (or other cause) has been ruled out; an examination may aggravate the condition.
Nursing Diagnoses
Ineffective Tissue Perfusion: Placental related to excessive bleeding causing fetal compromise.
Deficient Fluid Volume related to excessive bleeding.
Risk for Infection Related to operative intervention or delivery.
Anxiety related to excessive bleeding, procedures, and possible maternal-fetal complications.
Nursing Interventions
Promoting Tissue Perfusion
Monitor both the mother and fetus frequently; pulse, respirations, and BP should be taken as the patient’s condition warrants; continuous EFM if fetus viable.
Administer IV fluids, as prescribed.
Prepare for emergency delivery and neonatal resuscitation, as needed.
Maintaining Fluid Volume
Establish and maintain one or two large-bore IV lines, as needed; obtain CBC, type and screen/cross for blood replacement, platelets, PT/PTT, fibrinogen. Repeat periodically as patient’s condition warrants.
Assess bleeding periodically to note changes in frequency and volume.
Maintain strict bed rest during any bleeding episode in a lateral supine position.
If bleeding is profuse and delivery cannot be delayed, prepare for a cesarean delivery.
Administer blood component therapy, as necessary.
Preventing Infection
Use sterile technique when providing care.
Evaluate temperature and pulse periodically; if ruptured membranes, hypothermia, or hyperthermia, evaluate more frequently.
Evaluate white blood cell (WBC) and differential count.
Teach perineal care and handwashing techniques.
Assess for perineal odor after vaginal bleeding episodes.
Decreasing Anxiety
Explain all treatments and procedures; answer related questions to patient satisfaction.
Provide information on a cesarean delivery and prepare patient emotionally, if applicable.
Community and Home Care Considerations
Home care for patients with placenta previa and other antenatal bleeding disorders can occur if the following criteria are met:
No active bleeding.
No signs and symptoms of preterm labor (PTL).
Home close to medical facility.
Emergency support readily available.
Teach the woman signs and symptoms of hemorrhage; patient report to labor and delivery immediately if bleeding occurs.
Monitor vaginal discharge and bleeding after each urination and bowel movement.
Instruct the woman on home uterine activity monitoring, if ordered; use of palpation and electronic telemetry units included.
Instruct the woman on performing daily fetal movement counts (kick counts).
Antepartum testing may be increased, as indicated periodically.
Instruct the woman to have support persons readily available.
Instruct patient of the need for vaginal and sexual abstinence; discuss options.
Patient Education and Health Maintenance
Educate the woman and her family about the diagnosis, etiology, and treatment of placenta previa.
Educate the woman who is discharged from the hospital with placenta previa to avoid intercourse or inserting anything into her vagina, limit physical activity, have an accessible person in the event of an emergency, and report to the hospital immediately if repeat bleeding, more than six uterine contractions per hour, or decreased fetal movement.
Figure 39-3. Abruptio placentae— premature separation of the placenta.
Evaluation: Expected Outcomes
Fetal condition stable.
Absence of shock, stable vital signs, absence of bleeding.
Absence of signs or symptoms of infection.
Verbalizes concerns and understanding of procedures and treatments.
Abruptio Placentae
Abruptio placentae results from the premature separation of a normally implanted placenta before the birth of the fetus; typically occurs after 20 weeks’ gestation. Classifications include partial, complete, or marginal (Figure 39-3). Hemorrhage can be concealed (occult/hidden) or revealed (exposed). During an occult hemorrhage, the placenta detaches from the center, leaving the edges attached; this offers a concealed area for blood to pool behind the placenta. Even though bleeding is not evident at the perineum, concealed hemorrhage is accompanied by constant cramping or general abdominal pain. Prompt intervention is warranted.
Pathophysiology and Etiology
Typically, the etiology is unknown, but risks include:
History of abdominal trauma, prior cesarean birth, uterine anomalies (fibroids, septum).
Maternal hypertension: 50% of placental abruptions are associated with some form of hypertension.
Cigarette smoking, cocaine or amphetamine abuse.
Thrombophilias, such as Factor V Leiden or antiphospholipid antibody.
Previous history of abruptio placentae or partial abruption in current pregnancy.
Rapid decompression of the uterus (reduction of fluid with polyhydramnios).
Preterm premature rupture of membranes: less than 34 weeks.
Hemorrhage occurs into the decidua basalis behind the placenta and forms a hematoma. This hematoma will expand as bleeding increases; enlargement further detaches the placenta from the uterine wall.
Clinical Manifestations
Sudden-onset, intense, constant, generalized abdominal pain/tenderness with (revealed) or without (concealed) vaginal bleeding; approximately 10% of women present with concealed hemorrhage.
Uterine contractions are typically low amplitude and high frequency. Uterine baseline resting tone may be elevated over course of evolving abruption.
Changes in the FHR may commonly be the first sign of maternal hemodynamic imbalance. Category II or III patterns may evolve to include tachycardia or bradycardia, recurrent late decelerations with minimal or absent variability. Fetal response depends on amount of blood loss and extent of uteroplacental insufficiency present.
Patient may exhibit signs and symptoms of rapid labor progress and delivery.
Diagnostic Evaluation
Based on woman’s history, physical examination, laboratory studies, EFM data, and signs and symptoms to include vaginal bleeding, abdominal pain, uterine contractions, uterine tenderness, and/or maternal-fetal distress. Presentations vary per patient.
Ultrasound is performed to exclude placenta previa, but may not be sensitive enough to diagnose or rule out abruptio placentae; EFM is frequently more accurate.
Kleihauer-Betke lab test may be ordered to determine maternal-fetal hemorrhage by assessing maternal blood for the presence of fetal RBCs.
Management
Management depends on maternal and fetal status and degree of bleeding. Any viable fetus and patient with suspected abruptio placentae should be admitted immediately and continuous EFM applied.
In fetal compromise, severe hemorrhage, coagulopathy, or increasing uterine activity dysfunction, emergent cesarean delivery is highly recommended.
If the mother is hemodynamically stable and the fetus is stable (normal FHR/UA data) or has an intrauterine fetal demise, vaginal delivery may be recommended.
If mother is hemodynamically unstable, she may need stabilization with IV/blood/blood products replacement to maintain urine output and appropriate hematocrit levels. With rapid infusion of fluids, monitor woman for signs/symptoms of pulmonary edema.
A neonatal specialty team is necessary at delivery due to prematurity and neonatal complications.
Complications
Maternal shock, DIC.
Anaphylactoid syndrome of pregnancy (formerly amniotic fluid embolism).
Determine the amount and type of bleeding along with the presence or absence of pain; labor pain is episodic whereas placental abruption pain is constant.
Monitor maternal and fetal vital signs, especially maternal BP, pulse, FHR, FHR characteristics, and uterine activity data.
Palpate the abdomen.
Note presence of contractions and note relaxation between each subsequent contraction.
If contractions are not present, assess abdominal firmness (relaxed or tight).
Measure and record fundal height periodically to evaluate accumulation of concealed bleeding.
Prepare for possible delivery.
Table 39-2 Characteristics of Abruptio Placentae and Placenta Previa
CHARACTERISTIC
ABRUPTIO PLACENTAE
PLACENTA PREVIA
Onset
Third trimester
Third trimester (commonly at 32-36 weeks)
Bleeding
May be concealed, external dark hemorrhage, or bloody amniotic fluid
Mostly external, small to profuse in amount, bright red
Pain and uterine tenderness
Usually present; irritable uterus, progresses to boardlike consistency
Usually absent; uterus soft
Fetal heart tone
May be irregular or absent
Usually normal
Presenting part
May be engaged
Usually not engaged
Shock
Moderate to severe depending on extent of concealed and external hemorrhage
Usually not present unless bleeding is excessive
Delivery
Immediate delivery, usually cesarean delivery
Delivery may be delayed, depending on size of fetus and amount of bleeding
Nursing Diagnoses
Ineffective Tissue Perfusion: Placental related to excessive bleeding, hypotension, and decreased cardiac output, causing maternal-fetal compromise.
Deficient Fluid Volume related to excessive bleeding.
Fear related to excessive bleeding, procedures, and unknown outcome.
Nursing Interventions
Maintaining Tissue Perfusion
Evaluate amount of bleeding by weight of pads (actual blood loss) and direct visualization, rather than estimated blood loss, particularly if moderate to severe. Monitor CBC results and vital signs.
Position in the left lateral position, with head elevated.
Administer oxygen via face mask at 8 to 10 L/minute. Maintain oxygen saturation level above 90% to 95%. Limit prolonged use, particularly if delivery is imminent.
Evaluate fetal status with continuous external fetal monitoring.
Encourage relaxation techniques.
Prepare for possible cesarean delivery if maternal or fetal compromise is evident.
Maintaining Fluid Volume
Establish and maintain one to two large-bore IV lines for fluids and blood component therapy, as prescribed.
Evaluate coagulation studies and intake and output totals.
Monitor maternal vital signs and uterine activity.
Monitor vaginal bleeding and evaluate fundal height to detect an increase in bleeding.
Decreasing Fear
Inform the woman and her family about maternal-fetal status frequently.
Explain all procedures in advance when possible or as they are performed.
Answer questions in a calm manner, using simple terms.
Encourage the presence of a support person.
Patient Education and Health Maintenance
Provide information regarding etiology and treatment for abruptio placentae.
Encourage involvement from the neonatal team regarding education related to fetal/neonatal outcome.
Teach high-risk women the signs and symptoms of placental abruption.
Instruct woman to report to labor and delivery immediately should excessive bleeding or constant pain occur at home.
Instruct woman to have emergency plan in place for transport to medical facility. It is important to have support persons aware of procedures as well.
Evaluation: Expected Outcomes
FHR remains as Category I or II with minimal fetal deterioration noted.
Absence of shock, demonstrated by stable maternal vital signs after initiation of treatment.
Verbalizes concerns; asks questions.
Hypertensive Disorders of Pregnancy
Evidence Base
American College of Obstetricians and Gynecologists. (2002/Reaffirmed 2010). Diagnosis and management of preeclampsia and eclampsia (Practice Bulletin #33). Washington, DC: Author.
American College of Obstetricians and Gynecologists. (2011). Emergent therapy for acute-onset severe hypertension with preeclampsia and eclampsia (Committee Opinion
# 514). Washington, DC: Author.
Hypertensive disorders of pregnancy are considered the most common medical complications of pregnancy, affecting 12% to 22% of all pregnancies and responsible for 17.6% of maternal deaths in the United States. Classification varies from prepregnancy disease and beyond 12 weeks postpartum.
Classification
Chronic Hypertension
Hypertension is defined as mild—systolic BP ≥ 140 mm Hg or diastolic BP ≥ 90 mm Hg; or severe—systolic BP ≥ 180 mm Hg or diastolic BP ≥ 110 mm Hg. The condition may be observable before pregnancy, diagnosed before the 20th week of gestation, or persisting beyond 12 weeks postpartum. Condition increases risk of placental abruption.
Gestational Hypertension
New onset of hypertension (systolic BP ≥ 140 mm Hg or diastolic BP ≥ 90 mm Hg), generally after 20 weeks’ gestation in the absence of gestational proteinuria; replaces the term pregnancy-induced hypertension.
BP typically normalizes to prepregnancy values by 12 weeks postpartum; if it remains elevated past 12 weeks, then a diagnosis of chronic hypertension is confirmed.
Preeclampsia and Eclampsia
Preeclampsia—elevated BP accompanied by proteinuria (without evidence of urinary tract infection [UTI]); both must be present for a diagnosis.
Mild: systolic BP ≥ 140 mm Hg or diastolic BP ≥ 90 mm Hg on more than two occasions; gestational proteinuria > 300 mg on random specimen or >1+ on dipstick; urinary excretion ≥ 0.3 g protein in a 24-hour specimen (24-hour specimens are recommended for diagnosis).
Severe: diagnosis considered if preeclampsia evident and at least one of the following present: systolic BP ≥ 160 mm Hg; diastolic BP ≥ 110 mm Hg; proteinuria 5 g or >/24-hour specimen or 3+ on two or more random urine specimens; oliguria of <500 mL/24 hours, cerebral or visual disturbances, pulmonary edema or cyanosis, epigastric or right upper quadrant pain, impaired liver function, thrombocytopenia (<100,000/mm3 platelets), or fetal growth restriction.
HELLP syndrome—acronym stands for Hemolysis: microangiopathic hemolytic anemia, Elevated Liver Enzymes, and Low Platelets; form of severe preeclampsia (refer to Box 39-1).
Eclampsia—new onset of seizure activity or coma in a preeclamptic patient that cannot be attributed to any underlying neurologic condition or preexisting disease.
BOX 39-1 HELLP Syndrome
HELLP syndrome—consisting of Hemolysis of RBCs, Elevated Liver enzymes, and Low Platelets (<100,000 mm3)—is a severe complication with or without preeclampsia.
These findings are commonly associated with disseminated intravascular coagulation (DIC) and, in fact, may be diagnosed as DIC.
The hemolysis of erythrocytes is seen in the abnormal morphology of the cells.
The elevated liver enzyme measurement is associated with decreased blood flow to the liver as a result of fibrin thrombi.
The low platelet count is related to vasospasm and platelet adhesions.
Treatment is similar to treatment for preeclampsia with close monitoring of liver function and bleeding.
These women are at increased risk for postpartum hemorrhage.
Complaints range from malaise, epigastric pain, and nausea and vomiting to nonspecific viral syndrome-like symptoms.
Preeclampsia/Eclampsia Superimposed on Chronic Hypertension
Diagnosis based on presence of one or more of the following in woman with hypertension and proteinuria prior to 20 weeks’ gestation:
New onset of proteinuria.
Sudden increase in proteinuria.
Sudden increase in hypertension.
Development of HELLP syndrome.
Pathophysiology and Etiology
Etiologic theories include primary or excessive exposure to chorionic villi, as well as immunologic, genetic, and endocrine factors. These factors lead to endothelial dysfunction, systemic inflammatory response, and subsequent increased capillary permeability resulting in multisystem organ dysfunction. New research incorporates an allergic response from the mother against the fetus, similar to rejection of a transplanted organ. Hemoconcentration occurs due to vasoconstriction, increased vascular permeability, or both. Physiologic anemia results as a symptom due to decreased intravascular plasma volume.
The disease is more commonly seen in primigravidas.
Risk factors—chronic hypertension, hydatidiform mole, multiple gestation, polyhydramnios, preexisting vascular disease, obesity, and diabetes mellitus may predispose a patient to preeclampsia. Adolescents (younger than age 17) and women older than age 35 are at higher risk.
NURSING ALERT
The risk of preeclampsia is increased for multigravida women if they have a new partner (father of the baby different from previous children) due to new paternal genetic makeup of the fetus.
Diagnostic Evaluation
Evaluate BP with appropriate auditory sounds (Korotkoff Phase I-systolic and V-diastolic), cuff size (1.5 times circumference of upper arm), placement (arm resting at level of heart), and proper maternal position (sitting or semi-Fowler’s).
A 24-hour urine test is recommended for absolute diagnosis of preeclampsia.
Serum BUN, serum creatinine, and serum uric acid levels evaluate renal function and glomerular filtration capability, signaling advanced disease.
Liver function tests (AST, ALT); elevations indicative of organ dysfunction and disease.
Coagulation studies, specifically platelets, antithrombin III, and factor VIII levels.
Ultrasound assesses fetal growth, amniotic fluid volume, and placental implantation and function.
Periodic antepartum testing may be required to assess advanced or evolving disease and maternal-fetal tolerance: nonstress test (NST), oxytocin challenge test (OCT), biophysical profile (BPP).
Deep tendon reflexes and clonus evaluation assesses evolving disease and level of medications administered to treat disease.
Management
Treatment for hypertensive disorders of pregnancy focus on stabilization of the mother and pregnancy prolongation while observing for fetal intolerance. Delivery may be necessary for maternal indications, fetal indications, or both.
Expectant Management
Expectant management can be considered if the following maternal and fetal factors are present:
Maternal factors:
Controlled hypertension.
Urinary protein not severe; organ function adequate.
Oliguria (<0.5 mL/kg/hour) that resolves with hydration.
Liver enzymes not excessive, organ function adequate.
Fetal factors:
BPP > 6.
Amniotic fluid index (AFI) > 2 cm.
Ultrasound fetal weight > 5th percentile.
Delivery
Delivery may be considered if any of the following occur:
Maternal factors:
Uncontrolled hypertension: persistent > 160 systolic or 110 diastolic.
Eclampsia unresolved or controlled.
Thrombocytopenia: platelet count < 100,000/mm3.
Compromised liver function.
Pulmonary edema.
Compromised renal function.
Abruptio placentae.
Persistent and unresolved severe headache or visual changes.
Evidence of hemorrhagic stroke or coma.
Fetal factors:
Evolving Category II patterns or Category III FHR patterns (see page 1282).
BPP < 4 on two occasions, 4 hours apart.
AFI < 2 cm.
Ultrasound fetal weight less than 5th percentile.
Reverse umbilical artery diastolic flow.
Evidence of acute placental abruption.
Pharmacologic Therapies
Magnesium sulfate (MgSO4) is the primary medication for prophylactic treatment of seizure activity precipitated by hypertensive distress; may be given either via IV line or I.M., yet IV route is preferred; I.M. administration is reserved for eclamptic patients without IV access.
A 4-g loading dose of 50% MgSO4 is usually given via IV line over 15 to 30 minutes followed by a maintenance dose (secondary infusion) of 2 g/hour.
The therapeutic level for MgSO4 is a serum level of 4 to 7 mEq/dL. Periodic laboratory analysis of serum levels is required.
Actions: decreases neuromuscular irritability and blocks release of acetylcholine at the neuromuscular junction; depresses vasomotor center; depresses central nervous system (CNS) irritability.
Phenytoin, although proposed for eclampsia prophylaxis, is considered second-line therapy in the United States; preferred for patients with kidney dysfunction.
If seizures develop and the patient is not on MgSO4, 2 g may be given via IV line every 15 minutes to a maximum of 6 g or stabilization of patient. If patient has an existing MgSO4 infusion, give 1 to 2 g IV piggyback. Continue to check magnesium levels periodically to assess toxicity/therapeutic levels.
If seizures continue, paralytic agents may be necessary and the patient may require mechanical ventilation.
Calcium gluconate is maintained bedside (but must remain secure) as a reversal agent for magnesium toxicity; dosage is 1 g (10 mL of 10% solution) by slow IV push.
NURSING ALERT
Signs of MgSO4 toxicity include loss of deep tendon reflexes, including knee-jerk reflex, respiratory depression, oliguria, respiratory arrest, and cardiac arrest.
Antihypertensive Drug Therapy
Acute and persistent (> 15 minutes) onset of severe preeclampsia, systolic >160 or diastolic >110, is considered a hypertensive emergency warranting prompt medical management. A clinical relationship between severe systolic hypertension and risk of hemorrhagic stroke has been observed in pregnant and nonpregnant adults. Therefore, a systolic BP of 160 mm Hg or greater is widely adopted as the definition of severe hypertension in pregnant or postpartum women. The goal of antihypertensive therapy is not to achieve normotension but to reduce risk of stroke and coma. Blood pressure is maintained with a margin of safety (<100 mm Hg) without compromising adequate uterine perfusion.
Hydralazine—relaxes vascular arterioles and stimulates cardiac output via direct peripheral vasodilation.
Dosage: 5 to 10 mg IV push every 15 to 20 minutes to a maximum dose of 20 mg; dose cautiously and avoid hypotension.
Onset of action can occur in 10 to 20 minutes, with peak action in 20 minutes; duration of the drug can last 3 to 8 hours.
Monitor BP and pulse closely.
If desired response is not obtained after 20 mg, change agents or consider hemodynamic monitoring.
Adverse effects: flushing, headache, maternal and fetal tachycardia, palpitations, uteroplacental insufficiency with subsequent fetal tachycardia, late decelerations, and worsening hypertension (if due to elevated cardiac output). Rebound hypotension is possible if drug is given too rapidly.
Labetalol—alpha/beta-adrenergic blocker that decreases systemic vascular resistance without reflex tachycardia; it slows the maternal heart rate.
Contraindicated in women with asthma, heart failure, and/or second- or third-degree heart block.
Cardiac monitoring is required.
Administered as 20 mg IV bolus dose, followed by 40 mg if no effect is seen in 10 minutes, then 80 mg every 10 minutes to a maximum dose of 220 mg.
Onset of action is 1 to 2 minutes, with peak of action at 10 minutes; duration of drug effect lasts 6 to 16 hours.
Adverse effects: transient fetal and neonatal hypotension, bradycardia, and hypoglycemia. Small doses excreted in breast milk.
Complications
Complications of preeclampsia affect many organ systems to include cardiovascular, renal, hematologic, neurologic, hepatic, and uteroplacental.
Thrombocytopenia; acute liver dysfunction or failure.
Postpartum hemorrhage.
Blindness; retinal detachment.
Fetal intolerance of labor; evolving Category II or Category III patterns.
Hypoglycemia.
Hepatocellular dysfunction; hepatic rupture.
Prematurity.
Growth restriction and placental dysfunction.
Nursing Assessment
Evaluate BP with appropriate auditory sounds (Korotkoff Phase I-systolic and V-diastolic), cuff size (1.5 times circumference of upper arm), placement (arm resting at level of heart), and proper maternal position (sitting or semi-Fowler’s). Utilizing wrong size cuff may inadvertently increase or decrease BP.
Assess urine protein at the bedside and initiate a 24-hour urine specimen, as ordered.
Evaluate DTRs and clonus on admission and periodically throughout therapy.
Evaluate fetal status with NST, fetal movement (kick) counts, BPP, contraction stress test (CST) via nipple stimulation or OCT, and continuous EFM, as directed.
Evaluate uterine activity for high-frequency, low-intensity uterine contractions; possible signs and symptoms of PTL or placental abruption.
Periodically observe for signs and symptoms of advancing disease.
Monitor for signs of MgSO4 toxicity—absent knee-jerk reflex, respiratory depression, oliguria, absent FHR variability; if evident discontinue MgSO4 and notify health care provider immediately.
Monitor serum magnesium serum level every 24 hours or per facility’s policy.
Nursing Diagnoses
Risk for Fluid Excess Volume related to pathophysiologic aspects of disease leading to fluid overload.
Risk for Decreased Cardiac/Ineffective Cerebral Tissue Perfusion related to altered vascular perfusion caused by vasospasm and thrombosis formation.
Risk for Injury related to seizures, prolonged bed rest, or other therapeutic regimens.
Anxiety related to diagnosis and concern for self and fetus.
Deficient Diversional Activity related to prolonged bed rest.
Decreased Cardiac Output related to antihypertensive therapy.
Nursing Interventions
Maintaining Fluid Balance
Strict intake and output—control IV fluid intake using a continuous infusion pump. Utilize Foley catheter with urometer for adequate assessment of output. Notify health care provider if urine output is less than 25 mL/hour.
Monitor hematocrit levels to evaluate intravascular fluid status.
Monitor vital signs periodically as the patient’s condition warrants.
Auscultate breath sounds at admission and periodically; report signs of pulmonary edema (ie, wheezing, crackles, shortness of breath, increased pulse rate, increased respiratory rate, or reduced SpO2 saturation).
Promoting Adequate Tissue Perfusion
Position laterally to optimize maternal and placental perfusion.
Monitor fetal activity.
Evaluate NST and continuous EFM, if applicable, to determine fetal status.
Preventing Injury
Instruct patient on importance of reporting signs of advancing disease: headaches, visual changes, dizziness, respiratory distress, and/or epigastric pain.
Keep the environment quiet and calm as possible.
Hospitalized patients should have side rails remain up to prevent injury if seizure occurs.
Hospitalized patients should have oxygen, suction, and emergency medications immediately available for seizure management.
Assess DTRs and clonus periodically; increase frequency as patient’s condition warrants.
DRUG ALERT
Keep calcium gluconate at bedside as a reversal agent for magnesium toxicity. Dosage is 1 g (10 mL of a 10% solution) slow IV push. Be cautious with concurrent administration of opioids, CNS depressants, calcium channel blockers, and beta-adrenergic blockers.
Decreasing Anxiety and Increasing Knowledge
Explain disease process and care plan including signs and symptoms of evolving disease.
Discuss the effects of all medications on mother and fetus.
Allow time to ask questions and discuss feelings regarding the diagnosis and treatment plan.
Promoting Diversional Activities
Explain need for bed rest to the woman and her support persons.
Explore woman’s hobbies/diversional activities if prolonged hospitalization necessary.
Instruct family to arrange for community support (eg, church, women’s groups).
Maintaining Cardiac Output
Strict intake and output—control IV fluid intake using a continuous infusion pump. Utilize Foley catheter with urimeter for adequate assessment of output. Notify health care provider if urine output is less than 25 mL/hour.
Monitor maternal vital signs, especially mean BP, pulse, and respirations.
Assess formation of edema: peripheral and pulmonary. Report pitting edema of +2 or less or evidence of pulmonary edema to primary care provider immediately.
Monitor oxygenation saturation levels with pulse oximetry. Report rate of less than 95% to primary care provider.
Community and Home Care Considerations
Mild preeclampsia, if stable, may be considered for home care at the discretion of the primary practitioner.
Ensure patient has daily phone access to primary care provider.
Periodic home visits by nursing personnel may be warranted.
Teach woman signs and symptoms of evolving disease.
At-home BP monitoring requires use of same arm and same physical position (eg, on left side, on right side) during each assessment.
Assess urine protein status daily on the first voided urine or obtain 24-hour urine each week, as ordered.
Teach woman to assess daily fetal movement (kick) counts; arrange for weekly NST, if indicated.
Patient Education and Health Maintenance
Teach the woman the importance of bed rest.
Encourage support of family and friends; suggest diversional activities on bed rest.
Include support of the neonatal team for discussion of fetal prognosis with the woman and her family.
Evaluation: Expected Outcomes
BP and other vital parameters stable.
Absence of evolving Category II or Category III FHR patterns.
No seizure activity.
Expresses concern for self and fetus.
Maintains bed rest and pursues diversional activities.
No evidence of pulmonary edema; urine output adequate.
Polyhydramnios
Polyhydramnios or hydramnios is excess amniotic fluid; volume typically exceeds 1.5 to 2 L between 32 and 36 weeks’ gestation. About 50% of cases result in good outcomes.
Pathophysiology and Etiology
Amniotic fluid is 98% to 99% water, with the remainder consisting of proteins, carbohydrates, fats, electrolytes, enzymes, hormones, urinary by-products, fetal cells, lanugo, and vernix.
Volume facilitates normal lung and neuromuscular maturity.
At 36 weeks’ gestation, approximately 1 L of fluid is present with subsequent decreases over the duration of gestation.
The amount of amniotic fluid present is controlled in part by fetal urination and swallowing.
Polyhydramnios is idiopathic in 60% of women, but is associated with multiple gestation, immune and nonimmune hydrops fetalis, chromosomal anomalies such as Down syndrome, and fetal GI-cardiac-neural tube abnormalities.
Clinical Manifestations
Excessive weight gain, dyspnea.
Abdomen may be tense and shiny.
Edema of the vulva, legs, and lower extremities may be evident.
Increased uterine size for gestational age; usually accompanied by difficulty in palpating fetal parts or auscultation of the FHR.
Possible evolving Category II or Category III FHR patterns.
Diagnostic Evaluation
Ultrasound evaluation: AFI > 20 cm or single vertical depth pocket > 8 cm or total volume > 1.5 to 2L.
Difficult to palpate fetus or auscultate FHR.
Fundal height (FH) greater than age of gestation.
Management
Treatment is based on severity and underlying conditions; may include direct fetal therapy, serial amniocentesis, or administration of prostaglandin inhibitors such as indomethacin.
Indomethacin may be administered to increase fetal lung absorption, decrease fetal urine production, and increase fluid movement across the membranes of the mother.
Serial amniocentesis:
Fluid is slowly removed under ultrasound-guided needle aspiration; rapid removal can result in a premature separation of the placenta.
Usually 500 to 1,000 mL of fluid is removed during one procedure.
Complications
Potential for dysfunctional labor with increased risk for cesarean delivery.
Postpartum hemorrhage due to uterine atony from prolonged gross distention of the uterus.
Acute fetal hypoxia secondary to prolapsed cord or trauma.
Potential for preterm delivery.
Nursing Assessment
Evaluate maternal respiratory status; dyspnea may be present as hydramnios increases.
Evaluate EFM, continuously if viable, to assess fetal status.
Inspect abdomen and evaluate uterine height and compare with previous findings.
Evaluate for abdominal pain, edema, varicosities of lower extremities and vulva.
Nursing Diagnoses
Ineffective Breathing Pattern related to pressure on the diaphragm.
Impaired Physical Mobility related to edema and discomfort from the enlarged uterus.
Anxiety related to fetal outcome.
Risk for Bleeding at delivery related to prolonged overdistention of the uterus.
Nursing Interventions
Promoting Effective Breathing
Position to promote chest expansion with head elevated.
Provide oxygen (8 to 10 L/minute) by face mask, if indicated; prolonged use prior to delivery is not recommended.
Limit activities and plan for frequent rest periods.
Maintain adequate intake and output.
Promoting Mobility
Assist the woman with position changes and ambulation, as needed.
Advise on alternating activity with rest periods to promote circulation.
Instruct the woman to wear loose-fitting clothing and lowheeled shoes with good support.
Decreasing Anxiety
Explain probable causes of polyhydramnios, if known.
Encourage the patient and family to ask questions and express feelings regarding any treatment or procedure.
Prepare patient for mode of delivery that is anticipated and for the expected findings at the time of delivery.
Encourage presence and participation of support person in plan of care.
Preventing Hemorrhage during Labor
Notify primary care provider of inadequate or abnormal labor curve.
Place peripheral IV and maintain throughout labor with normal saline or dextrose (5%) in lactated Ringer’s solution (D5LR).
Administer medications (ie, oxytocin, misoprostol) to decrease postpartum bleeding, as necessary.
Observe for alterations in vital signs indicating excessive blood loss, such as decreasing BP and increasing pulse.
Medications for the prevention of postpartum hemorrhage should be immediately available following delivery (eg, oxytocin, misoprostol).
Patient Education and Health Maintenance
Instruct the woman to notify her health care provider if she experiences respiratory distress.
Teach the woman signs of PTL and importance to report them to health care provider.
Evaluation: Expected Outcomes
Only gold members can continue reading. Log In or Register to continue
 NURSING ALERT
NURSING ALERT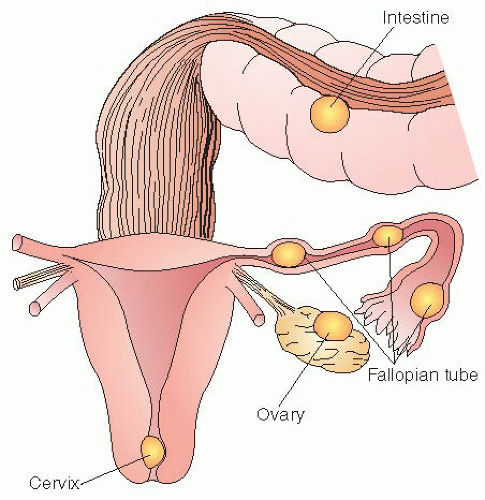
 NURSING ALERT
NURSING ALERT Evidence Base
Evidence Base Evidence Base
Evidence Base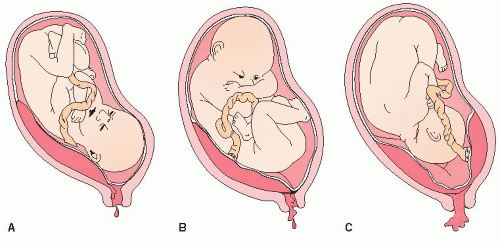
 NURSING ALERT
NURSING ALERT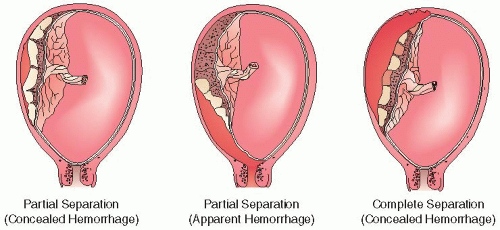
 Evidence Base
Evidence Base NURSING ALERT
NURSING ALERT NURSING ALERT
NURSING ALERT DRUG ALERT
DRUG ALERT


