The kidneys normally excrete a significant amount of acid on a daily basis. An impaired kidney, however, can neither excrete H
+ nor make extra HCO
3– for buffering. The amount of HCO
3– that exists is used up with the circulating acid. NH
4+ excretion, another method for eliminating acid, is also decreased due to the lack of available ions (see
Chapter 28). Because
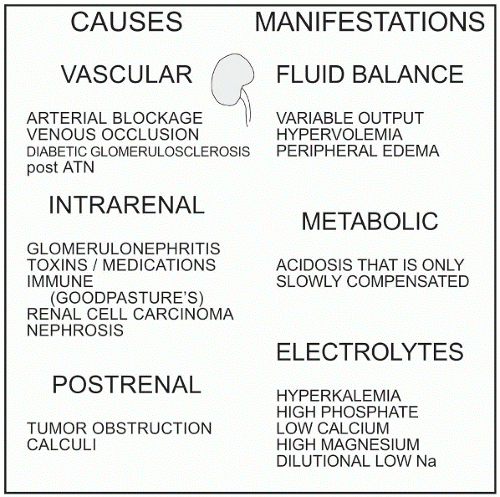
chronic renal failure is a slowly progressing disease, the body has time to compensate for the imbalance more easily than with an acute acidotic situation.
 The ability to clear urea and other metabolic products diminishes in chronic renal failure.
The ability to clear urea and other metabolic products diminishes in chronic renal failure.


