Cholelithiasis, Cholecystitis, and Related Disorders
The most common biliary tract disease, cholelithiasis is the formation of stones or calculi (gallstones) in the gallbladder. The prognosis is usually good with treatment unless infection occurs. In that case, the prognosis depends on the infection’s severity and its response to antibiotics. The formation of gallstones can give rise to a number of related disorders.
In cholecystitis, the gallbladder becomes acutely or chronically inflamed, usually because a gallstone becomes lodged in the cystic duct, causing painful gallbladder distention. The acute form is most common during middle age; the chronic form, among elderly persons. The prognosis is good with treatment.
In choledocholithiasis, gallstones pass out of the gallbladder and lodge in the common bile duct, causing partial or complete biliary obstruction. The prognosis is good unless infection occurs.
In cholangitis, the bile duct becomes infected; this disorder is commonly associated with choledocholithiasis and may follow percutaneous transhepatic cholangiography. Nonsuppurative cholangitis usually responds rapidly to antibiotic treatment. Suppurative cholangitis has a poor prognosis unless surgery to correct the obstruction and drain the infected bile is performed promptly.
In gallstone ileus, a gallstone obstructs the small bowel. Typically, the gallstone travels through a fistula between the gallbladder and small bowel and lodges at the ileocecal valve. This condition is most common in elderly persons. The prognosis is good with surgery.
Generally, gallbladder and duct diseases occur during middle age. Between ages 20 and 50, they’re six times more common in females, but the incidence in males and females equalizes after age 50. The incidence rises with each succeeding decade.
Where calculi collect
Possible locations for calculi include these sites.
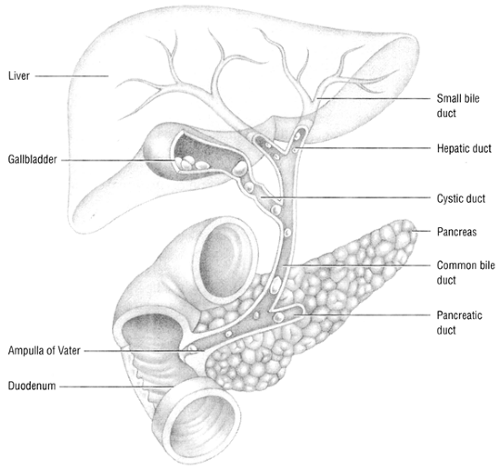 Figure. No caption available |
Causes
These related disorders all stem from a common cause: formation of calculi. Although the exact cause of gallstone formation is unknown, abnormal metabolism of cholesterol and bile salts clearly plays an important role.
A number of risk factors have been identified that predispose a person to calculi formation. These include:
a high-calorie, high-cholesterol diet, associated with obesity
elevated estrogen levels from oral contraceptive use, postmenopausal hormone-replacement therapy, or pregnancy
the use of clofibrate
diabetes mellitus, ileal disease, hemolytic disorders, hepatic disease, or pancreatitis.
The disorder that develops depends on where in the gallbladder or biliary tract the calculi collect. For example, cholelithiasis results when gallstones form and remain in the gallbladder. Cholecystitis, choledocholithiasis, cholangitis, and gallstone ileus usually develop after a gallstone lodges in a duct or in the small bowel, causing an obstruction. (See Where calculi collect.)
Complications
Each of these disorders produces its own set of complications.
Cholelithiasis may lead to any of the disorders associated with gallstone formation: cholangitis, cholecystitis, choledolithiasis, and gallstone ileus.
Cholecystitis can progress to gallbladder complications, such as empyema, hydrops or mucocele, or gangrene. Gangrene may lead to perforation, resulting in peritonitis, fistula formation, pancreatitis, or porcelain gallbladder. Other complications include chronic cholecystitis and cholangitis.
Choledocholithiasis may lead to cholangitis, obstructive jaundice, pancreatitis, and secondary biliary cirrhosis.
Cholangitis may progress to septic shock and death, especially in the suppurative form.
Gallstone ileus may cause bowel obstruction, which can lead to intestinal perforation, peritonitis, septicemia, secondary infection, and septic shock.



