Central nervous system (CNS) malignancies occur in the brain or spinal cord; they may be primary or metastatic.
A. Incidence: Approximately 18,300 people will be diagnosed with new cases of primary CNS malignancies each year in the United States, and over 13,000 will die. More than 100,000 new cases of metastatic CNS tumors are diagnosed each year in the United States. CNS tumors are more common in whites and, except for meningiomas, occur more often in men than women. The incidence of CNS tumors appears to be increasing in the elderly population; improved techniques are responsible for much of the increase in diagnoses over the last 30 years.
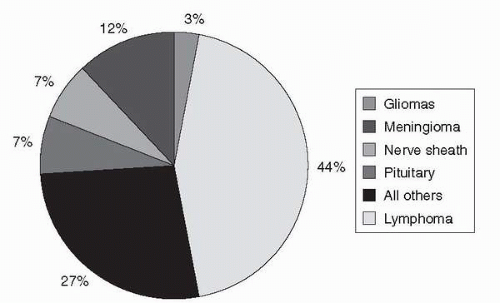
B. Primary brain tumors include more than 100 histologic classifications and grades (Figure 11-1).
1. The most common are gliomas (astrocytomas, oligodendrogliomas, ependymomas).
2. Astrocytomas, the most common glial tumor, are graded from I to IV, low to high grade. High-grade astrocytomas, anaplastic astrocytomas, and glioblastoma multiforme occur most frequently and carry the worst prognosis.
3. Survival and prognosis in adults are more favorable if patients have a low-grade tumor, are under age 40, have a high performance status (70% on the Karnofsky scale), and receive a good surgical resection.
C. Metastatic tumors
1. The brain is a common site of metastases for many cancers, including lung, breast, colon, renal, and melanoma.
2. Signs and symptoms are the same as primary brain lesions.
3. Prognosis is best for patients with solitary lesions, good performance ratings (70% on the Karnofsky scale), age <60 years, and primary tumor in remission.
4. Metastatic lesions are treated with surgery, whole brain radiation, or stereotactic radiosurgery. The number, size, and location of the lesions, as well as the patient’s condition and primary disease status, will determine which modality is used.
D. Spinal cord tumors are less common than other CNS tumors. Symptoms depend on the location of the lesion. Surgery or radiation therapy or both are used to cure, control, or palliate disease.
II. Etiology:
Although the causes of some CNS tumors are unknown, many genetic and environmental factors are being considered. Factors such as previous exposure to ionizing radiation and chemicals, viral infections, and low-frequency electromagnetic fields are possible; however, questions still prevail. Similarities in environmental exposure are thought to explain clustering of CNS tumors in families.
Figure 11-1. Incidence of primary brain tumors by tissue diagnosis (CBTRUS, 2002).
III. Patient Management
A. Assessment: Signs and symptoms of CNS tumors depend on the type of tumor, size, location in the brain, and the extent of increased intracranial pressure (ICP). Symptoms are caused by the disturbance or destruction of brain tissue secondary to tumor invasion, infiltration, and compression.
1. Many patients with CNS tumors present with similar general nonfocal symptoms such as cognitive changes, headaches, or seizures caused by increased ICP.
2. Other patients present with localizing signs, specific to the location of the tumor (Table 11-1).
3. A complete history and physical, neurologic examination, and family history are required to identify symptoms and establish baseline function. If cognitive ability is impaired, someone who knows the patient well can often assist in identification of specific symptoms and time of onset.
B. Diagnostic Parameters
1. Magnetic resonance imaging (MRI) detects brain and spinal abnormalities and reveals abnormalities in the nature and extent of tumor blood flow. The scan can last from 45 minutes (brain only) to 3 hours (cranial-spinal axis). Patients are required to lie in a loud, confined space, which may be problematic for claustrophobics, although open scanners address this issue. Intravenous (IV) contrast (gadolinium) is usually given. In contrast-enhanced scans, the disrupted tumor vasculature allows contrast dye to cross the blood-brain barrier (BBB) and is clearly visible on the scan. MRI is the standard evaluation for brain cancers; advantages include greater sensitivity than the computed tomography (CT) scan without ionizing radiation. Disadvantages include expense, potential patient anxiety, rare but possible reactions to contrast, and inability to scan patients with metal foreign bodies (due to effects of the magnet).
TABLE 11-1 CNS Tumor Signs
Anatomic Location
Deficit/Abnormality
Frontal
Personality/behavior changes, emotional lability, short-term memory deficits, impaired intellect and judgment, expressive aphasia, contralateral motor weakness, seizures, and urinary incontinence
Contralateral sensory disturbances (hyperesthesia, paresthesia, astereognosis, autotopagnosia); visual field defects; left-right discrimination; difficulty with language, writing, and calculations; and seizures
Occipital
Visual field deficits (vision loss in half of each visual field on side opposite the lesion), blindness, visual hallucinations, seizures, and difficulty naming objects
Cerebellum
Problems with gait, balance, and coordination; nystagmus; signs of increased ICP caused by obstruction of CSF flow
Hypothalamus
Endocrine dysfunction, temperature control malfunction, abnormal thirst and appetite, emotional lability
Decreased level of consciousness; abnormal heart rate, respirtions, blood pressure, swallowing, vomiting; sensory motor impairment, cranial nerve deficits
2. CT scans have replaced more invasive diagnostic tests due to safety and accuracy. The CT scan can detect brain and spine abnormalities, including masses and edema. When the procedure is done on a high-speed multislice scanner, it requires several minutes to complete and IV contrast is usually given. Advantages include three-dimensional pictures viewed with special computers and the ability to visualize bony abnormalities and blood. Risks include the use of ionizing radiation and reactions to contrast media, although the new contrast agents are safer and produce fewer reactions.
3. Positron emission tomography (PET) measures regional brain metabolism and blood flow by tracing positron-emitting radionuclides. The procedure requires about 2 hours and an arterial line. PET scans are used to try to differentiate between active recurrent tumor and tumor necrosis by measuring the rate of glucose metabolism. Disadvantages include possible arterial line complications.
4. Single photon emission computed tomography (SPECT) is used to differentiate tumor growths from benign or necrotic lesions. The procedure is similar to a bone scan and requires about 1 hour. SPECT uses conventional radio tracers.
5. MRI spectroscopy (MRS) is functional MRI that studies numerous brain metabolites. Like PET, MRS can differentiate between necrotic tissue and active tumor. It is a useful diagnostic tool, and recent technologic advances have simplified its use in a clinical setting. No contrast agents are used; scanning parameters and postprocessing determine which metabolites are imaged. Disadvantages are that a spectroscopic scan adds about 20 minutes to the standard MRI examination.
6. Definitive diagnosis is determined by obtaining tissue, either during craniotomy or by biopsy. In certain areas of the brain where it is not safe to obtain tissue, diagnosis is presumed by evaluating imaging, patient history, and clinical assessment.
C. Treatment: Multimodal treatment of adult primary brain tumors usually includes surgery, with the addition of radiation therapy, chemotherapy, or all three for more aggressive tumors (Table 11-2). Chapters 6, 8, and 9 review common side effects and general management of patients treated with these therapies.
1. Surgical debulking of primary brain tumors defines pathology, decreases tumor mass and ICP, and may relieve neurologic symptoms.
a. Surgery of accessible tumors is a safe procedure and usually well tolerated.
b. Potential surgical complications include increased ICP leading to herniation, hemorrhage, local/regional brain damage, and cranial nerve injury. Complications are secondary to tissue damage and related to the area of tumor location.
c. Potential postoperative complications include postoperative hematomas, infection, spinal fluid leaks, meningitis, deep venous thrombosis (DVT), and pulmonary embolism.
2. Radiation therapy is a localized treatment and requires individualized planning. External beam radiation is used to treat primary and metastatic brain tumors and some histologically benign brain tumors.
a. Treatment planning considers histology, grade, location, radio responsiveness, intent, and patient status.
b. Specialized techniques (eg, interstitial brachytherapy, stereotactic radiosurgery, gamma knife and proton beam particle delivery) allow radiation to be delivered with precision to the tumor. As a result, limited exposure of normal cells results in fewer complications and side effects. These techniques are not appropriate for all tumor types.
Only gold members can continue reading. Log In or Register to continue