Hospitalization of a child brings about a range of emotions in the child and his or her family. In order to care for the hospitalized child, one must take into consideration the child’s development and family coping skills. Being hospitalized versus receiving care at home affects the child’s response to his or her illness. In addition, family presence is often an integral part of pediatric patient care. Facilitating family-centered care allows the family to fully support the child during his or her hospitalization. Knowledge of these aspects will assist the registered nurse in providing appropriate pediatric patient care.
Pain Management
Evidence Base
Habich, M., Wilson, D., Thielk, D., et al. (2012). Evaluating the effectiveness of pediatric pain management guidelines. Journal of Pediatric Nursing—Nursing Care of Children & Families, 27(4), 336-345.
Accurate assessment and timely management of pain in children is an important and challenging nursing responsibility because infants and young children cannot express their pain, as adults can.
General Considerations
Pain experienced by infants and children is not effectively identified or managed in many cases.
There are still misunderstandings about the ways pain is experienced and expressed by infants and children.
Behavioral and physiologic cues are used to assess pain in infants. Special rating tools are available to involve children in assessing the intensity of their pain, including the Pain Experience Inventory, CRIES Neonatal Postoperative Pain Measurement Scale, Oucher Pain Rating Scale, Numerical or Visual Analog Scale, FLACC Behavioral Pain Assessment Scale, and the Wong-Baker FACES Pain Rating Scale (see Figure 43-1).
Pain caused by a condition is not always proportional to the seriousness of the illness or injury. For example, a relatively minor illness, such as an earache, is a very painful experience, whereas an enlarging tumor may not cause pain in early stages.
It is important to consider pain when a child is noncommunicative, has decreased consciousness, is intubated, or whose chosen language is not understood by the health caregivers.
It is equally important to consider pain when a child requires an injection, blood test, or noninvasive or invasive diagnostic test.
Figure 43-1. Wong-Baker FACES Pain Rating Scale. (Hockenberry, M. J., & Wilson, D. (2012). Wong’s essentials of pediatric nursing (9th ed.). Philadelphia: Elsevier.)
Consider parents when assessing and managing the pain of their child. It is well documented that parents are important influences on their children.
Consider the way in which the parents view the situation experienced by the child and work with them to intervene effectively.
Presence of the parents during a procedure can be very positive, especially when the family has been prepared.
At other times, it is recommended that the parents mutually agree to wait in a nearby area.
Arbitrary rules against parental presence are often designed to meet the needs of staff, not the needs of the child and his or her parents.
Nursing Interventions
Anticipate pain and intervene early.
Use a rating scale that the child can understand and use it consistently with that child for initial pain assessment and to determine the effectiveness of interventions. Attempt to introduce the pain rating scale to the child prior to the surgery or procedure.
Use self as therapeutic presence to help ease pain.
Teach self-regulation and self-control techniques.
Utilize distraction by sounds, music, audio images, and movies.
Allow self-soothing maneuvers (thumbsucking, clinging to blanket, rocking).
Reposition patient, as needed.
Decrease environmental light and noise when possible.
Consider referral for self-hypnosis and conscious relaxation techniques.
Utilize medication delivered by way of noninvasive routes where possible.
Administer premedication—anesthetizing, anti-anxiety, and anti-emetic medications, as indicated.
Assist with conscious sedation when indicated, following standards of practice related to assessment, staffing, care, and documentation.
Reassess the patient’s response to the intervention and document appropriately. This is important to evaluate effectiveness and identify possible new pain issues.
The Child Undergoing Surgery
Evidence Base
Vincent, C., Chiappetta, M., Beach, A., et al. (2012). Parents’ management of children’s pain at home after surgery. Journal for Specialists in Pediatric Nursing, 17(2), 108-120.
Physical and emotional preparation for surgery will minimize stress and will help the child and family cope effectively with surgery. Also see Chapter 7, Perioperative Nursing.
Psychological Preparation and Support
Potential threats for the hospitalized child anticipating surgery are:
Separation from parents; peers for the older child or adolescent.
The strange and unknown—possibility of surprise.
Confusion and uncertainty about limits and expected behavior.
Relative loss of control of their world, loss of autonomy.
Fear of anesthesia.
Fear of the surgical procedure itself.
Misinterpretation of medical jargon (eg, dye/die).
The attitudes of the parents toward hospitalization and surgery largely determine the attitudes of their child.
The experience may be emotionally distressing.
Parents may have feelings of fear or guilt.
The preparation and support should be integrated for parent, child, and family unit.
Give individual attention to parents; explore and clarify their feelings and thoughts; provide accurate information and appropriate reassurance.
Stress parents’ importance to the child. Help parents understand how they can care for their child.
Preoperative Teaching
All preparation and support must be based on the child’s age, developmental stage, and level; personality; past history and experience with health professionals and hospitals; background including religion, socioeconomic circumstances, culture, and family attitudes and dynamics. Anxiety level and coping skills should be taken into consideration.
Inquire as to what information the child has already received.
Determine what the child knows or expects; identify family myths and possible misunderstandings.
Additional guidelines in preparation include:
Use illustration or model of a child’s body, concrete examples, and simple terms (not medical jargon).
Identify changes that may occur as a result of the procedure, both in body and daily routine.
Give explanations slowly and clearly, saving anxiety-producing aspects until the end. Repeat as needed.
Make use of the child’s creative ability and logical thinking powers to aid in preparation for procedures.
Involve parents, as indicated, depending on the situation.
Allow and encourage the child to participate as able.
Suggest ways for the child to cope—crying is okay.
Offer constant reassurance; speak in a calm manner.
Evaluate the child’s understanding of your teaching. Repeat and correct information, as necessary.
Orient the patient and family to the unit, room, location of playroom, operating room and recovery room (if applicable) and introduce them to appropriate personnel. Make arrangements for the child to meet the anesthesiologist as well as the operating room nurse and recovery room nurse.
Allow and encourage questions. Give honest answers.
Such questions will give the nurse a better understanding of the child’s fears and perceptions of what is happening.
Infants and young children need to form a trusting relationship with those who care for them.
The older the child, the more reassuring information can be.
Provide opportunity for the child and parents to work out concerns and feelings (play, talk). Such supportive care should result in less upset behavior and more cooperation.
Prepare the child for what to expect postoperatively (ie, equipment to be used or attached to child, where the child will wake up, how the child will feel, what the child will be expected to do, diet, any physical restrictions). Be honest about what pain they may experience.
Educate parents regarding the option to be with their child, if available at the facility, during induction of anesthesia to reduce separation anxiety and fear.
Physical Preparation
Assist with necessary laboratory studies. Explain to the child what is going to happen before the procedure and how he or she may respond. Give continual support during the procedure.
See that the patient has nothing by mouth (NPO). Explain to the child and his or her parents what NPO means and the importance of it. Place signs on the patient’s hospital door indicating the NPO status to ensure that non-family members and non-staff members do not give the patient food.
Assist with fever reduction.
Fever can result from some surgical problems (eg, intestinal obstruction).
Fever increases risk of anesthesia and need for fluids and calories.
Administer appropriate medications, as prescribed. Sedatives and drugs to dry the secretions are often given on the unit preoperatively.
Establish good hydration. Parental therapy may be necessary to hydrate the child, especially if the child is NPO, vomiting, or febrile.
With the parents in attendance, assist the surgeon with marking the patient’s intended surgical site, as recommended by The Joint Commission as part of the National Safety Goals.
Allow the child to carry a toy or other comfort item to the preoperative area.
Immediate Postoperative Care
Maintain a patent airway and prevent aspiration.
Position the child as ordered depending on his or her surgical procedure; position as needed to allow secretions to drain and to prevent the tongue from obstructing the pharynx.
Suction any secretions present. Avoid causing a gag reflex or spasm during suctioning.
Make frequent observations of general condition and vital signs. Postoperative protocols may vary per procedure and facility.
Take vital signs every 15 minutes until the child is awake and his or her condition is stable.
Note temperature, respiratory rate and quality, pulse rate and quality, blood pressure, skin color.
Watch for signs of shock.
Children in shock may have signs of pallor, coldness, increased pulse, and irregular respiration.
Older children have decreased blood pressure and respiration.
Change in vital signs may indicate airway obstruction or compromise, hemorrhage, atelectasis, altered hemodynamics.
Restlessness may indicate pain or hypoxia. Medication for pain is not usually given until anesthesia has worn off. Give analgesics and sedatives per the pain management team orders.
Check dressings for drainage, constriction, and pressure. Perform dressing changes per protocol.
See that all drainage tubes are connected and functioning properly. Gastric decompression relieves abdominal distention and decreases the possibility of respiratory compromise. Chest tubes evacuate pleural air and fluid. Ensure all tubes are secure to prevent accidental removal.
Monitor parenteral fluids, as prescribed.
Be physically near as the child awakens to offer soothing words and a gentle touch. Reunite the parents and child as soon as possible after the child recovers from anesthesia. If a language barrier exists, the parents should be with the child during recovery from anesthesia and an interpreter should be present when medical explanations are being given to the parents or child.
After Recovery from Anesthesia
After undergoing simple surgery and receiving a small amount of anesthesia, the child may be ready to play and eat in a few hours. More complicated and extensive surgery debilitates the child for a longer period of time.
Continue to make frequent and astute observations in regard to behavior, comfort level and pain control, vital signs, dressings or operative site, and special apparatus (intravenous [IV] lines, chest tubes, oxygen, nasogastric tubes).
Note signs of dehydration—dry skin and membranes; sunken eyes; poor skin turgor; sunken fontanelle in an infant; poor urine output.
Record any passage of flatus or stool and bowel sounds. Observe for intestinal ileus because crying children swallow air, which may cause gastric distention.
Record vomiting time, amount, and characteristics.
Assess behavior for signs of pain and medicate appropriately.
Record intake and output accurately.
Parenteral fluids and oral intake.
Drainage from gastric tubes or chest tubes, colostomy, wound, and urinary output.
Parenteral fluid is evaluated and prescribed by considering output and intake. It is usually maintained until the child is taking adequate oral fluids.
Advance diet as tolerated, according to the child’s age and the health care provider’s directions.
First feedings are usually clear fluids; if tolerated, advance slowly to full diet for age. Note any vomiting or abdominal distention.
Because anorexia may occur, offer what the child likes in small amounts and in an attractive manner.
Prevent infection.
Keep the child away from other children or personnel with respiratory or other infections.
Change the child’s position every 2 to 4 hours; support infant with a blanket roll.
Encourage the child to cough and breathe deeply; let the infant cry for short periods of time, unless contraindicated. Offer older children incentive spirometry every hour while awake.
Keep operative site clean—change dressing, as ordered; in infant, keep the diaper away from the wound.
Enforce diligent handwashing by family members and staff before any contact with the patient.
Do not cohort surgical patients with patients with a proven or presumptive infection.
Administer prophylactic antibiotics, as ordered.
Provide good general hygiene and opportunities for exercise and diversional activity; encourage sleep and rest.
Provide emotional support and psychological security. Reassure the child that things are going well; if there are complications, offer honest information based on the patient’s health and developmental level and the parents’ willingness to share this information with their child. Talk about going home, if appropriate.
Begin early to prepare for discharge: teach special procedures, provide written instructions, and arrange for community nurse referral.
Table 43-1 Stages of Dying as ldentified by Dr. Elizabeth kübler-Ross
STAGE
NURSING CONSIDERATIONS
I. Denial, shock, disbelief
• Accept denial, but function within a reality sphere. Do not tear down the child’s (or family’s) defenses.
• Be aware that denial usually breaks down in the early morning when it may be dark and lonely.
• Be certain that it is the child or family who is using denial, not the staff.
II. Anger, rage, hostility
• Accept anger and help the child express it through positive channels.
• Be aware that anger may be expressed toward other family members, nursing staff, physicians, and other persons involved.
• Help families recognize that it is normal for children to express anger for what they are losing.
III. Bargaining (from “No, not me,” to “Yes, me, but …”)
• Recognize this period as a time for the child and family to regain strength.
• Encourage the family to finish any unfinished business with the child. This is the time to do things such as take a promised trip or buy a promised toy.
IV. Depression (The child and/or family experiences silent grief and mourns past and future losses.)
• Recognize this as a normal reaction and expression of strength.
• Help families to accept the child who does not want to talk and excludes help. This is the usual pattern of behavior.
• Reassure the child that you can understand his or her feelings.
V. Acceptance
• Assist families to provide significant loving human contact with their child and one another.
The Dying Child
The nursing role is to assist the child and family to cope with the experience in such a way that it will promote growth rather than destroy family integrity and emotional well-being.
Recognize the Stages of Dying
Evidence Base
Kubler-Ross, E. (1997). On death and dying. New York: Scribner.
Nielson, D. (2012). Discussing death with pediatric patients: Implications for nurses. Journal of Pediatric Nursing, 27(5), e59-64.
Be aware that dying children, their families, and the staff will all progress through these stages, not necessarily at the same time.
Children experience the stages with much variation. They tend to pass more quickly through the stages and may merge some of these stages.
The nursing goal is to accept the child and his or her family at whatever stage they are experiencing, not to push them through the stages.
Understand the meaning of illness and death at various stages of growth and development (see Table 43-2).
Be aware of other factors that influence a child’s personal concept of death. Of particular importance are:
The amount and type of direct exposure a child has had to death.
Cultural values, beliefs, and patterns of bereavement.
Religious beliefs about death and an afterlife.
Meet with the parents separately from the child and discuss their wishes regarding dissemination of information to their child.
Table 43-2 Stages in the Development of a Child’s Concept of Death
AGE OF CHILD
STAGE OF DEVELOPMENT
Child up to age 3
• At this stage, the child cannot comprehend the relationship of life to death because the child has not developed the concept of infinite time.
• The child fears separation from protecting and comforting adults.
• The child perceives death as a reversible act.
Preschool child
• At this age, the child has no real understanding of the meaning of death; the child feels safe and secure with parents.
• The child may view death as something that happens to others.
• The child may interpret the separation that occurs with hospitalization as punishment; the painful tests and procedures that the child is subjected to support this idea.
• The child may become depressed because of not being able to correct these wrongdoings and regain the grace of adults.
• The concept may be connected with magical thoughts of mystery.
School-age child
• The child at this age sees death as the cessation of life; child understands that he or she is alive and can become “not alive”; child fears dying.
• The child differentiates death from sleep. Unlike sleep, the horror of death is in pain, progressive mutilation, and mystery.
• The child is vulnerable to guilt feelings related to death because of difficulty in differentiating death wishes and the actual event.
• The child believes death may be caused by angry feelings or bad thoughts.
• The child learns the meaning of death from own personal experiences, such as the death of pets, family members, and public figures.
• Television and movies have contributed to the concept of death and understanding of the meaning of illness. There may be more knowledge in the meaning of the diagnosis and an awareness that death may occur violently.
Adolescent
• The adolescent comprehends the permanence of death as the adult does, although the adolescent may not comprehend death as an event occurring to persons close to self.
• The adolescent wants to live—sees death as thwarting pursuit of goals: independence, success, achievement, physical improvement, and self-image.
• The adolescent fears death before fulfillment.
• The adolescent may become depressed and resentful because of bodily changes that may occur, dependency, and the loss of social environment.
• The adolescent may feel isolated and rejected because adolescent friends may withdraw when faced with impending death of a friend.
• The adolescent may express rage, bitterness, and resentment; especially resents the fact that fate is to die.
Communicate with the Child about Death
Research indicates that children generally can cope with more than adults will allow and that children appreciate the opportunity to know and understand what is happening to them. It is important that the child’s questions be answered simply but truthfully. The answers should be based on the child’s particular level of understanding. The following responses have been suggested by Easson in The Dying Child: The Management of the Child or Adolescent Who Is Dying and may be useful as a guide:
Preschool-Age Child
When the child at this age is comfortable enough to ask questions about illness, questions should be answered. When death is anticipated at some future time and the child asks “Am I going to die?”, a response might be, “We will all die someday, but you are not going to die today or tomorrow.”
When death is imminent and the child asks “Am I going to die?”, the response might be, “Yes, you are going to die, but we will take care of you and stay with you.”
When the child asks “Will it hurt?”, the response should be truthful and factual.
Death should never be described as a form of sleep. Some children may fear sleep as the result of this type of explanation. Anesthesia is sometimes called a “special sleep” so it is not currently recommended to refer to death as “sleep.”
Parents can express to the child the fact that they do not want the child to go and that they will miss the child very much; they feel sad, too, that they are going to be separated.
School-Age Child
Responses to the school-age child’s questions about death should be answered truthfully. The child looks for support from those he or she trusts.
The school-age child should be given a simple explanation of his or her diagnosis and its meaning; the child should also receive an explanation of all treatments and procedures.
The child should be given no specific time in terms of days or months because each individual and each illness is different.
When the school-age child asks “Am I going to die?” and death is inevitable, the child should be told the truth. The school-age child has the emotional ability to look to parents and those he or she trusts for comfort and support.
The school-age child believes in his or her parents. The child should be allowed to die in the comfort and security of his or her family.
The school-age child knows death means final separation and knows what will be missed. The child must be allowed to mourn this loss. The dying child may be sad and bitter and demonstrate aggressive behavior. The child must be allowed the opportunity to verbalize this if able to do so.
Adolescent
The adolescent should be given an explanation of his or her illness and all necessary treatments and procedures.
The adolescent feels deprived and reasonably resentful regarding his or her illness because he or she wants to live and reach fulfillment.
As death approaches, the adolescent becomes emotionally closer to his family.
The adolescent should be allowed to maintain emotional defenses—including absolute denial. The adolescent will indicate by questions what types of answers are desired.
If the adolescent states, “I am not going to die,” he or she is pleading for support. Be truthful and state, “No, you are not going to die right now.”
The adolescent may ask, “How long do I have to live?” Adolescents are able to face reality more directly and can tolerate more direct answers. No absolute time should be given because that blocks all hope. If an adolescent has what is felt to be a prognosis of approximately 3 months, the response might be, “People with an illness like yours may die in 3 to 6 months, but some may live much longer.”
Support Parents’ Adaptation to Child’s Death
Develop a care plan that includes this approach:
The primary responsibility for communicating with the parents should be designated to one nurse.
Information regarding the parents’ concerns should be communicated to all staff members and should be included in the patient’s care plan.
Accept parental feelings about the child’s anticipated death and help parents deal with these feelings.
It is not unusual for parents to reach the point of wishing the child dead and to experience guilt and self-blame because of this thought.
The parents may withdraw emotional attachments to the child if the process of dying is lengthy. This occurs because the parents complete most of the mourning process before the child reaches biologic death. They may relate to the child as if he or she were already dead.
Provide anticipatory guidance regarding the child’s actual death and immediate decisions and responsibilities afterward.
Describe what the death will probably be like and how to know when it is imminent. This is necessary to dispel the horrifying fantasies that many parents have. Reassure the parents that all measures will be taken to keep the child comfortable at the time of death. (Note: Certain diseases, despite appropriate medical interventions, may cause an uncomfortable or painful death. Parents should be promised complete comfort for their child only if this expectation is realistic.)
Clarify the parents’ wishes about being present at the child’s death and respect their desires. See if they want to hold the child—before, during, or after the death.
If appropriate, allow the parents to discuss their feelings about issues such as autopsy and organ donation in order that they may make appropriate decisions. Do not make them feel guilty if they do not consent.
If necessary, assist the parents to think about funeral arrangements.
Be aware of factors that affect the family’s capacity to cope with fatal illness, especially social and cultural features of the family system, previous experiences with death, present stage of family development, and resources available to them.
Contact the appropriate clergy if the family desires. Contact other extended family members for support if they wish.
During final hours, do not leave the family alone, unless they request it.
Encourage parents and siblings to share their thoughts with the dying child.
Provide information on bereavement support groups, usually available through hospital or church.
PEDIATRIC PROCEDURES
Restraints
Evidence Base
Crellin, D., Babl, F., Sullivan, T., et al. (2011). Procedural restraint use in preverbal and early-verbal children. Pediatric Emergency Care, 27(7), 622-627.
Protective measures to limit movement may be necessary for restraining children in the health care setting (see Figure 43-2). They can be a short-term restraint to facilitate examination and minimize the child’s discomfort during special tests, procedures, and specimen collections. Restraints can also be used for a longer period of time to maintain the child’s safety and protection from injury.
Figure 43-2. Types of restraints.
General Considerations
Protective devices should be used only when necessary and after all other considerations are exhausted, never as a substitute for careful observation of the child.
Protective devices cannot be used on a continuous basis without an order. Continuous use requires justification and full documentation of the type of restraint used, reason for use, and the effectiveness of the restraint used. Ongoing monitoring, documentation, and renewal of the order, with the length of time the restraint will be in place, are required.
The reason for using the protective device should be explained to the child and parents to prevent misinterpretation and to ensure their cooperation with the procedure. Children often interpret restraints as punishment.
Teach the child and family about specific devices they may be using in the hospital (ie, side rails) and after discharge (ie, mitts, elbow restraints).
Any protective device should be checked frequently to make sure it is effective and is not causing any ill side effects. It should be removed periodically to prevent skin irritation or circulation impairment. Provide range of motion and skin care routinely.
Do not cover an IV site with a restraint when possible.
Protective devices should always be applied in a manner that maintains proper body alignment and ensures the child’s comfort.
Any protective device that requires attachment to the child’s bed should be secured to the bed springs or frame, never the mattress or side rails. This allows the side rails to be adjusted without removing the restraint or injuring the child’s extremity.
Any required knots should be tied in a manner that permits their quick release. This is a safety precaution.
When a child must be immobilized, an attempt should be made to replace the lost activity with another form of motion. For example, although restrained, a child can be moved in a stroller, wheelchair, or in bed. When arms are restrained, the child may be allowed to play kicking games. Water play, mirrors, body games, and blowing bubbles are helpful replacements.
Restraints should be removed as soon as the child is no longer considered a danger to self or others or when medical devices are no longer in place.
NURSING ALERT
An order from a health care provider is needed to initiate continuous restraints. Proper documentation is required when restraints are in use. Do not secure restraints to bed rails or mattresses. Hourly assessment of the restrained extremity is needed to ensure there has been no impairment of circulation and constriction or respiratory compromise with chest restraints.
Mummy Device
The mummy device involves securing a sheet or blanket around the child’s body in such a way that the arms are held to the sides and leg movements are restricted (see Figure 43-2). This short-term type of restraint is used on infants and small children during treatments and examinations involving the head and neck.
Equipment
Small sheet or blanket.
Nursing Action
Place the blanket or sheet flat on the bed.
Fold over one corner of the blanket.
Place the child on the blanket with shoulder at the edge of the fold.
Pull the right side of the blanket firmly over the child’s right shoulder.
Tuck the remainder of the right side of the blanket under the left side of the child’s body.
Repeat the procedure with the left side of the blanket.
Separate the corners of the bottom portion of the sheet and fold it up toward the child’s neck.
Tuck both sides of the sheet under the child’s body.
Secure by crossing one side over the other in the back and tucking in the excess, or by pinning or taping the blanket in place.
Special Precautions
Make certain the child’s extremities are in a comfortable position during this procedure. Make sure that the restraint is not obstructing the child’s airway.
Jacket Device
The jacket device is a piece of material that fits the child like a jacket or halter. Long tapes are attached to the sides of the jacket (see Figure 43-2). Jacket device restraints are used to keep the child in a wheelchair, high chair, or crib.
Nursing Action
Put the jacket on the child so the opening is in the back.
Tie the strings securely with a knot that can be easily released, if necessary.
Position the child in a wheelchair, high chair, or crib.
Secure the long tapes appropriately:
Under the arm supports of a chair.
Around the back of the wheelchair or high chair.
To the springs or frame of a crib.
Special Precautions
Children in cribs must be observed frequently to make certain they do not become entangled in the long tapes of the jacket device. Release, reposition, and perform range of motion exercises as per hospital policy.
Belt Device
The belt device is exactly like the jacket method of restraining, except that the material fits the child like a wide belt and buckles in the back (see Figure 43-2).
Elbow Device
The elbow device is a plastic device that fits around the arm at the elbow bend and is secured with a Velcro strap. This type of restraint prevents flexion of the elbow. It is especially useful for pediatric patients receiving IV therapy, those with eczema or other skin rashes, and those following a cleft lip repair, eye surgery, or any other type of procedure or surgery in which touching the upper extremities, head, or neck should be prevented.
Equipment
Elbow device.
Skin protective material for under the device (long-sleeved shirt or gauze).
Nursing Action
Cover the elbow with a long-sleeved shirt or gauze if irritation or sweating is expected.
Place the child’s arm in the center of the appropriately sized elbow restraint.
Wrap the restraint around the child’s arm.
Secure with Velcro.
Special Precautions
The child’s fingers should be observed frequently for coldness or discoloration and the skin under the device should be checked for signs of irritation.
The device should be removed periodically according to facility policy or standards of care to provide skin care and range of motion.
Devices to Limit Movement of the Extremities
Many different kinds of devices are available to limit motion of one or more extremities. One commercial variety consists of a piece of material with tapes on both ends to be secured to the frame of the bed. The material also has two small flaps sewn to it for securing the child’s ankles or wrists. Similar devices are available that use sheepskin flaps. These should be used when the device will be necessary over a prolonged period or for children with sensitive skin. This restraining device may be used to restrain infants and young children for procedures, such as IV therapies and urine collection.
Equipment
Extremity restraint of appropriate size for the child (small, medium, or large).
Nursing Action
Secure the device to the crib or bed frame.
Velcro the small flaps securely around the child’s ankles or wrists.
Special Precautions
The child’s fingers or toes should be observed frequently for coldness or discoloration and the skin under the device should be checked for signs of irritation.
The device should be removed periodically according to policy or standards of care to provide skin care and range of motion exercises and documentation should be completed.
Abdominal Device
The abdominal device is used for restraining a small child in a crib. It operates exactly like the method described for limiting the movements of extremities. However, the strip of material is wider and has only one wide flap sewn in the center for fastening around the child’s abdomen.
Mitts
Mitts are used to prevent a child from injuring self with his or her hands and from removing tubes or IV lines. They are especially useful for children with dermatologic conditions such as eczema or burns and for those with nasogastric or nasojejunal feeding tubes. Mitts can be purchased commercially or made by wrapping the child’s hands in Kling gauze or by covering the child’s hands with a pair of clean socks and securing them to the wrist with tape.
NURSING ALERT
Mitts should be removed at least every 4 hours to permit skin care and to allow the child to exercise fingers.
Crib Top Device
A crib top device is used to prevent an infant or small child from climbing over the crib sides. Several types of commercial devices are available, including nets, plastic tops, and domes. A crib top device should be applied to the crib of a child capable of climbing over the crib sides (usually between ages 1 and 4).
NURSING ALERT
In all instances, it is essential to be certain that the crib sides are kept all of the way up and latched securely.
Papoose Board
A papoose board is the most cumbersome restraint device that may be used for procedures of the head, chest, and abdomen. Straps restrain the child or infant at the forehead, lower arms, and thighs (see Figure 43-2, page 1452).
Specimen Collection
Evaluation of specimens such as blood, urine, and stool is important in determining the status of the child. The nurse should be adept in the techniques for obtaining specimens, as well as meticulous in labeling and recording them.
For catheterization of the urinary bladder, refer to Chapter 21. For infants and children, the catheter size is 6 to 10 F, depending on the size of the child.
Heyland, D., Cahill, N., Dhaliwal, R., et al. (2010). Impact of enteral feeding protocols on enteral nutrition delivery: Results of a multicenter observational study. Journal of Parenteral and Enteral Nutrition, 34(6), 675-684.
Nutritional requirements may increase while infant or child is ill, but the ability to feed naturally may be impaired by illness or the child’s response to illness. If existing feeding patterns cannot be maintained, alternate methods may be necessary. The ability to feed enterally is preferred over parenteral nutrition due to decreased risk of complications as well as improved physiological response.
Gavage feeding is a means of providing food by way of a catheter passed through the nares or mouth, past the pharynx, down the esophagus, and into the stomach, slightly beyond the cardiac sphincter. Feedings may be continuous or intermittent.
Gavage feedings can provide a method of feeding or administering medications that require minimal patient effort when the child is unable to suck or swallow adequately.
Gavage feedings can be used to administer supplemental calories to a patient who is unable to meet their caloric needs by mouth. They also can be used to provide full calories to those unable to tolerate oral intake.
Gavage feedings can prevent fatigue or cyanosis that can occur from bottle-feeding in susceptible infants. They can provide supplements for an infant who is a poor bottle-feeder.
Gavage feedings can provide a safe method of feeding patients with hypotonia, patients experiencing respiratory distress, patients with uncoordinated suck and swallow, patients that are intubated, patients with a debilitation, and patients with anomalies of the digestive tract.
PROCEDURE GUIDELINES 43-1
Assisting with Blood Collection
EQUIPMENT
23- to 19-gauge short needle or scalp vein needle
Smaller volume or micro bloodcollecting tubes
Antiseptic wipes (alcohol)
Warm compresses
Smaller tourniquet (rubber band may be used with infant)
Gloves per standard precautions
Band-aid or pressure dressing
PROCEDURE
Nursing Action
Rationale
Preparatory phase
1.
Perform hand hygiene.
1.
Standard precautions.
2.
Immobilize the child by placing in a mummy restraint, if necessary or use distraction techniques.
2.
Allows easier access to the venipuncture site and protects child from injury.
3.
Position the patient.
3.
These positions allow for optimal visualization and stabilization of the patient.
a.
Femoral venipuncture: Place child on back with legs in froglike position. Place your hands on the child’s knees.
Assisting with jugular venipuncture.
a.
Cover perineum to protect site in case child voids.
Assisting with antecubital fossa venipuncture.
b.
External jugular venipuncture: Place the child in mummy restraint and lower head over the side of the bed or table. Turn head to side and stabilize. (See accompanying figure.)
b.
Crying will make external jugular vein visible and causes blood to flow more readily.
c.
Antecubital fossa venipuncture: Place the child in a supine position. The nurse stands on the side opposite the site to be used (across from the person drawing the specimen). The nurse positions her right arm across the upper part of the child’s chest and grasps the shoulder at the axilla position. The nurse’s left arm is placed across the lower part of the child’s chest and is used to extend the child’s arm at the wrist (see accompanying figure). If possible, allow child to sit upright while being held by parent to decrease stress of child and parent.
c.
The nurse’s hands are used to straighten and hold the child’s arm still; arms are used to maintain stability of child’s upper body.
d.
Infant—heel, toe, or digital puncture: Warm area with warm compress for 5-10 minutes.
d.
This dilates vessels, allowing blood to flow more freely, and reduces bruising.
1.
Capillary: Clean area with antiseptic and dry with sterile 2” × 2” gauze. Hold heel firmly and with free hand quickly puncture with microlancet or sterile 21-gauge needle on most medial or lateral part of plantar surface. Puncture deeply enough to get free-flowing blood—never deeper than 2 mm. Discard first drop of blood; rapidly collect specimen in proper capillary tube.
1.
Standard precautions. Both persons holding the infant and drawing the blood should wear gloves. Gowns, masks, and goggles may be used if splattering is anticipated.
2.
After the specimen is collected and the needle is removed, apply pressure to the site with dry gauze for 3-5 minutes.
2.
The femoral and jugular veins are large vessels. Because intravascular pressure is great, bleeding, oozing, and hematoma formation may result. External pressure prevents this from happening.
a.
Jugular venipuncture: While applying pressure to the site, place the patient in an upright sitting position. Do not apply excessive pressure that may compromise circulation or respiration.
a.
Upright position will reduce pressure in jugular vein.
3.
When the bleeding has stopped, apply a pressure dressing or adhesive bandage to the site. Soothe and comfort the child before leaving.
3.
Crying and thrashing about may initiate bleeding.
Follow-up phase
1.
Check the patient frequently for 1 hour after the procedure for oozing, bleeding, or evidence of a hematoma.
Key Decision Point
Anticipate bleeding if venipuncture was difficult. Hold pressure over the area until oozing has stopped (longer if the child is being treated with aspirin or an anticoagulant). Assess frequently and reapply pressure, if needed; report continued oozing or hematoma formation.
2.
Record carefully and accurately:
2.
For continuity of care.
a.
Site of venipuncture
b.
How the patient tolerated procedure
c.
Bleeding stopped or continued and for how long
d.
Test for which the specimen was collected as well as the place to which it was sent for analysis and the time at which it was sent
e.
Amount of blood loss
Evidence Base Bowden, V. R., & Greenberg, C. S. (2011). Pediatric nursing procedures (3rd ed.). Philadelphia: Lippincott Williams & Wilkins.
Gastrostomy Feeding
Only gold members can continue reading. Log In or Register to continue
 Evidence Base
Evidence Base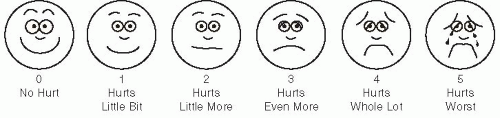
 Evidence Base
Evidence Base Evidence Base
Evidence Base Evidence Base
Evidence Base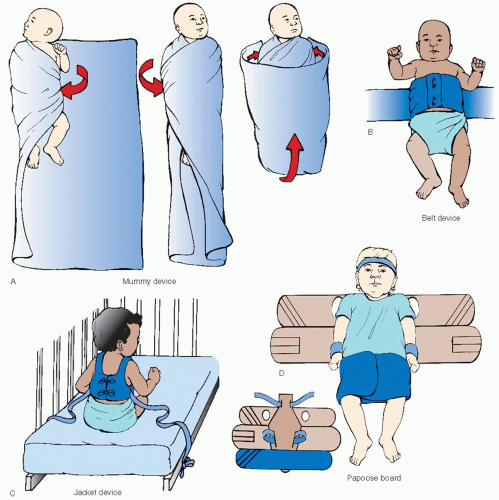
 NURSING ALERT
NURSING ALERT NURSING ALERT
NURSING ALERT NURSING ALERT
NURSING ALERT Evidence Base
Evidence Base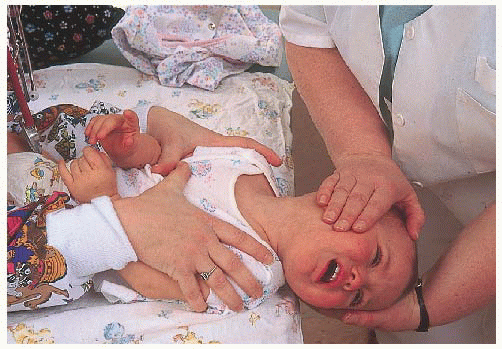 Assisting with jugular venipuncture.
Assisting with jugular venipuncture.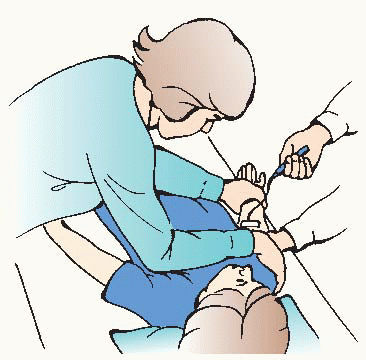 Assisting with antecubital fossa venipuncture.
Assisting with antecubital fossa venipuncture. Key Decision Point
Key Decision Point Evidence Base Bowden, V. R., & Greenberg, C. S. (2011). Pediatric nursing procedures (3rd ed.). Philadelphia: Lippincott Williams & Wilkins.
Evidence Base Bowden, V. R., & Greenberg, C. S. (2011). Pediatric nursing procedures (3rd ed.). Philadelphia: Lippincott Williams & Wilkins.


