Care of Mother and Neonate During the Postpartum Period
Care of Mother and Neonate During the Postpartum Period
NURSING CARE OF THE MOTHER
The Puerperium
The puerperium is the period beginning after delivery and ending when the woman’s body has returned as closely as possible to its prepregnant state. The period lasts approximately 6 weeks. (See Standards of Care Guidelines 38-1, page 1296.)
Physiologic Changes of the Puerperium
Evidence Base
Cunningham, F. G., Leveno, K. J., Bloom, S. L. et al. (2010). The puerperium. In Williams obstetrics (23rd ed., pp. 646-660). New York: McGraw-Hill.
Whitmer, T. (2011). Physical and psychologic changes. In S. Mattson & J. E. Smith (Eds.), Core curriculum for maternal-newborn nursing (4th ed., pp. 301-314). St. Louis, MO: Saunders Elsevier.
Uterine changes.
Immediately after delivery, the fundus is palpable halfway between the umbilicus and symphysis pubis. At 1 hour postpartum, the fundus is usually level with or slightly below the level of the umbilicus. The fundus is usually midline. Within 12 hours of delivery, the fundus may be ½ inch (1.3 cm) above the umbilicus and by 24 hours, ¼ inch (1 cm) below the umbilicus. After this, the level of the fundus descends approximately 1 fingerbreadth (or ½ inch) each day, until by the 10th to the 14th day, it has descended into the pelvic cavity and can no longer be palpated (see Figure 38-1).
After delivery, lochia—a vaginal discharge that consists of fatty epithelial cells, shreds of membrane, decidua, and blood—is red or dark brown with clots (lochia rubra) for approximately 1 to 3 days. It then progresses to a paler pink or more brown-tinged color of serosanguineous consistency (lochia serosa) for 3 to 10 days, followed by a whitish or yellowish color (lochia alba) in the 10th to 14th day. Lochia usually ceases by 3 weeks and the placental site is completely healed by the 6th week.
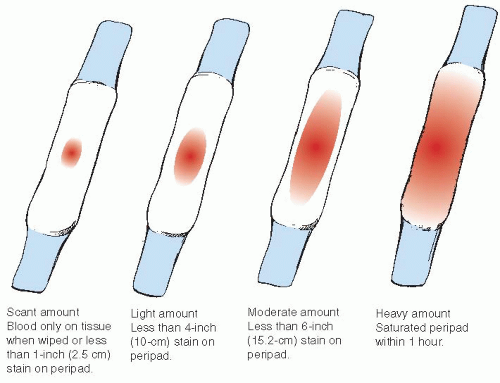
The amount of lochial flow can be scant (less than 2.5 cm stain [1 inch]/hour), light (less than 10 cm stain [4 inches]/hour), moderate (less than 15.2 cm stain [6 inches]/hour), or heavy (one pad saturated within 1 hour). Lochial flow is considered to be “excessive” if the perineal pad becomes saturated in less than 15 minutes (see Figure 38-2).
Immediately after delivery of the placenta, the cervix has little tone or resemblance to the prepregnant state. In approximately 2 to 3 days, it appears more like the prepregnant state and is dilated to 2 to 3 cm. By the end of the first postpartum week, it is approximately 1 cm in diameter. The cervical opening is more slitlike than the prepregnant dimple and remains that way. The cervical opening does not return to the prepregnant dimple following delivery unless the cervix has never been dilated.
Figure 38-1. Changes in uterine size and shape following delivery. (A) Uterus after delivery. (B) Uterus at 6th day. (C) Nongravid uterus.
The vaginal walls, uterine ligaments, and muscles of the pelvic floor and abdominal wall regain most of their tone during the puerperium. Immediately after delivery, the vaginal walls are smooth and swollen because the vaginal rugae are absent. Rugae reappears approximately 3 weeks postpartum. At approximately 6 weeks postpartum, involution of the vagina is complete.
Postpartum diuresis begins within 12 hours after birth and continues for 2 to 5 days postpartum, as extracellular water accumulated during pregnancy is excreted. Diuresis may also occur shortly after delivery if urine output was obstructed because of the pressure of the presenting part, or if IV fluids were given during labor.
Breasts.
With loss of the placenta, circulating levels of estrogen and progesterone decrease and levels of prolactin increase, thus initiating lactation in the postpartum woman.
Colostrum—a thick, yellowish fluid that contains more minerals and protein but less sugar and fat than mature breast milk and has a laxative effect on the infant—is secreted for the first 2 days postpartum.
Mature milk secretion is usually present by the third postpartum day, but may be present earlier if a woman breast-feeds immediately after delivery. Usually by the end of the second postpartum week mature breast milk is present.
Breast engorgement with milk, venous and lymphatic stasis, and swollen, tense, and tender breast tissue may occur between day 3 and day 5 postpartum.
Endocrine/metabolic function.
Human chorionic gonadotropin declines rapidly and is nonexistent by the end of the first postpartum week.
Thyroid levels are normal by 4 to 6 weeks postpartum.
Glucose levels are low secondary to decreased human placental lactogen, decreased Cortisol, decreased estrogen, and decreased growth hormone. Blood glucose levels of women with gestational (type 2) diabetes may return to normal limits shortly after birth.
Figure 38-2. Assessing the volume of lochia by peripad saturation.
Ovarian function.
Estrogen and progesterone levels decrease rapidly after delivery of the placenta and are usually their lowest by the seventh postpartum day.
Estrogen reaches the follicular phase by 3 weeks after birth, as long as the woman is not lactating.
Ovulation may occur as early as 27 days after delivery. The average time is 70 to 75 days postdelivery and 190 days postdelivery if breastfeeding.
The start of menses after delivery is individualized. Usually, the first menses occurs approximately 7 to 9 weeks after delivery in non-nursing mothers, although breastfeeding women may not start their first menses until as late as 18 months.
Kidneys and bladder function.
Mild proteinuria (+1 on urine dipstick) is common for 1 to 2 days after delivery in 40% to 50% of postpartum women.
Spontaneous voiding should return by 6 to 8 hours postpartum. Bladder tone returns between 5 and 7 days postpartum.
The catabolic process of involution can cause an increase in blood urea nitrogen levels during the postpartum period.
Stress incontinence is common during the first 6 weeks postpartum.
Neurologic function.
Discomfort and fatigue are common.
Afterpains and discomfort from the delivery, lacerations, episiotomy, and muscle aches are common for the first 2 to 3 days postdelivery.
Frontal and bilateral headaches are common and are caused by fluid shifts in the first week postpartum.
Non-rapid-eye-movement (REM) sleep is absent after birth and increases during the next 2 weeks. REM sleep decreases as non-REM sleep increases.
Carpal tunnel syndrome (resulting from physiologic edema causing pressure on the median nerve) is usually relieved by postpartum diuresis.
Cardiovascular function.
Most dramatic changes occur in this system and can take between 6 and 12 weeks to return to the prepregnant state.
Cardiac output peaks to about 80% immediately after birth (10 to 15 minutes) then decreases rapidly, reaching prelabor values by about 1 hour postpartum. However, it can remain elevated for as much as 48 hours postpartum. Cardiac output values return to normal by 2 to 3 weeks postpartum.
Hematocrit increases and increased red blood cell (RBC) production stops.
Leukocytosis with increased white blood cells (WBCs) common during the first postpartum week.
Respiratory function.
Returns to normal by approximately 6 to 8 weeks postpartum.
Basal metabolic rate increases for 7 to 14 days postpartum, secondary to mild anemia, lactation, and psychological changes.
Partial pressure of arterial oxygen (PaO2), partial pressure of carbon dioxide (PaCO2), and pH usually return to normal by 3 weeks postpartum.
GI/hepatic function.
GI tone and motility decreases in the early postpartum period, commonly causing gaseous distention of the abdomen and constipation.
Normal bowel function, including normal bowel movements, returns at about 2 to 3 days postpartum.
Liver function returns to normal approximately 10 to 14 days postpartum.
Gallbladder contractility increases to normal, allowing for expulsion of small gallstones.
Musculoskeletal function.
Generalized fatigue and weakness is common.
Decreased abdominal tone is common.
Diastasis recti heals and resolves by the 4th to 6th week postpartum. Until healing is complete, usually 1 to 2 weeks postpartum, abdominal exercises are contraindicated.
Joint instability returns to normal between 6 and 8 weeks postpartum.
Integumentary function.
Striae lighten and melasma is usually gone by 6 weeks postpartum.
Hair loss can increase for the first 4 to 20 weeks postpartum and then regrowth will occur, although the hair may not be as thick as it was before pregnancy.
A good method to remember how to check the postpartum changes is the use of the acronym BUBBLERS:
B—Breast.
U—Uterus.
B—Bladder.
B—Bowel.
L—Lochia.
E—Episiotomy.
R—Emotional response.
S—Homans’ sign.
STANDARDS OF CARE GUIDELINES 38-1
Postpartum Care
Perform assessment regularly for BUBBLERS—breasts, uterus size and consistency, bladder distention, bowel elimination, lochia, episiotomy, emotional response, and Homans’ sign.
Notify health care provider immediately if abnormalities are present:
Increased respiration and pulse, decreased blood pressure, and orthostatic changes may indicate hemorrhage.
Excessive vaginal bleeding (saturation of peripad within 1 hour for 2 or more hours), expulsion of large clots, or steady increase in vaginal bleeding, which indicates hemorrhage.
Boggy uterine fundus that does not become firm and remain firm with massage, indicating uterine atony.
Inability to void and bladder distention, which may displace uterus, leading to uterine atony.
Decreased urine output, which may indicate hemorrhage.
Elevated temperature, increased pain, swelling, and redness from incisions, indicating infection.
Calf tenderness, swelling, redness, or warmth, which may indicate a blood clot.
Excessive irritability, crying, moodiness, withdrawal, insomnia, and loss of interest in activities, which may indicate postpartum depression.
Encourage rest, nutrition, and bonding with the infant.
Provide education on feeding, bathing, changing, safety measures, signs of illness, and when to call infant’s pediatric care provider with questions.
This information should serve as a general guideline only. Each patient situation presents a unique set of clinical factors and requires nursing judgment to guide care, which may include additional or alternative measures and approaches.
NURSING ALERT
Hematuria immediately after normal spontaneous vaginal birth is usually indicative of bladder trauma. If hematuria occurs after the first 24 hours, it is indicative of urinary tract infection (UTI).
NURSING ALERT
Postpartum eclamptic seizures can begin more than 48 hours and less than 4 weeks postdelivery. They are commonly preceded by severe headache or vision disturbances (spots before the eyes, double vision, etc.). Extra care is taken to observe for these symptoms, especially in women with prenatal diagnosis of preeclampsia or hypertension.
NURSING ALERT
A positive Homans’ sign may indicate thrombophlebitis and should be reported to the primary care provider. The woman should be instructed not to massage her legs.
Emotional and Behavioral (Psychosocial) Status
Evidence Base
American College of Obstetricians and Gynecologists. (2008/Reaffirmed 2009). Use of psychiatric medications during pregnancy and lactation (Practice Bulletin #92). Washington, DC: Author.
Bigelow, A., Power, M., MacLellan-Peters, J., et al. (2012). Effect of Mother/Infant Skin-to-Skin Contact on Postpartum Depressive Symptoms and Maternal Physiological Stress. Journal of Obstetric, Gynecologic, & Neonatal Nursing, 41(3), 369-382.
Segre, L. S., O’Hara, M. W., Amdt, S., et al. (2011). Screening and counseling for postpartum depression by nurses: The women’s views, part 2. Maternal Child Nursing, 35(4), 220-225.
After delivery, the woman may progress through Rubin’s stages of taking in, taking hold, and letting go.
Taking in (extends over first 24 hours postpartum:
May begin with a refreshing sleep after delivery. Restorative sleep should occur within first 24 hours postdelivery.
Woman exhibits passive, dependent behavior.
Woman is concerned with sleep and the intake of food, mainly for herself.
Taking hold (if not in first 24 hours postpartum then between days 2 and 4 postpartum):
Woman begins to initiate action and to function more independently. First sign mother is in this phase is alert interest in her infant.
Woman may require more explanation and reassurance that she is functioning well, especially in caring for her infant.
Openness to teaching on care of self and neonate.
Today, with early hospital discharge, this phase may occur earlier, or it may occur after discharge.
Letting go:
Begins near the end of the first week; no specific end time noted.
Is influenced by cultural beliefs.
Reestablishment of couple relationship.
As the woman meets success in caring for the neonate, her concern extends to other family members and to their activities.
Some women may experience euphoria in the first few days after delivery and set unrealistic goals for activities after discharge from the birthing place.
Many women may experience temporary mood swings during this period because of the discomfort, fatigue, and exhaustion following labor and delivery and because of hormonal changes after delivery.
Up to 50% to 75% of mothers may experience postpartum (or maternity) blues. They can last for a few hours to 1 to 2 weeks and usually peak at approximately the 5th postpartum day. Women may exhibit irritability, poor appetite, insomnia, tearfulness, or crying. This is a normal reaction to the physiologic shifts that occur postdelivery and is a temporary situation.
Postpartum depression is a more serious problem. Research shows that women feel a loss of control of all aspects of life and go through a four-stage process that includes: encountering terror, dying of self, struggling to survive, and regaining control.
Nursing research findings indicate that new mothers commonly identify postpartum needs such as coping with:
The physical changes and discomforts of the puerperium, including a need to regain their prepregnancy figure.
Changing family relationships and meeting the needs of family members, including the infant.
Fatigue, emotional stress, feelings of isolation, and being tied down.
A lack of time for personal needs and interests.
Nursing Assessment
Evidence Base
Cunningham, F. G., Leveno, K. J., Bloom, S. L., et al. (2010). The puerperium. In Williams obstetrics (23rd ed., pp. 646-660). New York: McGraw-Hill.
Intermountain Utah Valley Regional Medical Mother/Baby Unit. (2010). Assessment of the new mother & baby [DVD/CD]. Salt Lake City, UT: Concept Media.
Immediate Postpartum Assessment
The first hour after delivery of the placenta (fourth stage of labor) is a critical period; postpartum hemorrhage is most likely to occur at this time (see page 1364).
Subsequent Postpartum Assessment
Check firmness of the fundus at regular intervals. Perform fundal massage if the uterus is boggy (not firm) (see Figure 38-3).
Figure 38-3. Fundal massage. With hands correctly positioned, gentle fundal massage stimulates the uterine muscles to contract, helping to restore normal tone and control bleeding.
Inspect the perineum regularly for frank bleeding.
Note color, amount, and odor of the lochia.
Count the number of perineal pads that are saturated in each 8-hour period.
Assess vital signs at least twice daily and more frequently, if indicated.
Assess bowel and bladder elimination.
Evaluate interaction and care skills of the mother and family with infant.
Assess for breast engorgement and condition of the nipples if breastfeeding.
Inspect legs for signs of thromboembolism and assess Homans’ sign.
Assess incisions for signs of infection and healing.
A good method to remember how to evaluate the episiotomy is the use of the acronym REEDA:
R—Redness.
E—Edema.
E—Ecchymosis (purplish patch of blood flow).
D—Discharge.
A—Approximation, or the closeness of the skin edges.
REEDA is based on a 3-point scale. A score of 3 indicates an assessment of very poor wound healing. On the first postpartum day, the REEDA score may range from 0 to 3; by the second postpartum week, the score should be 0 to 1.
If the patient is Rh negative, evaluate her need for Rho(D) immune globulin (RhoGAM). If indicated, administer the RhoGAM within 72 hours of delivery.
If the woman is not rubella immune, a rubella vaccination may be given and pregnancy must be avoided for at least 3 months.
Nursing Management
Evidence Base
Bond, L. (2011). Physiology of pregnancy. In S. Mattson & J. E. Smith (Eds.), Core curriculum for maternal-newborn nursing (4th ed., pp. 80-100). St. Louis, MO: Saunders Elsevier.
Rhode, M. A. (2011). Postpartum complications. In S. Mattson & J. E. Smith (Eds.), core curriculum for maternal neonatal nursing (4th ed., pp. 650-666). St. Louis, MO: Saunders Elsevier.
Nursing Diagnoses
Risk for Deficient Fluid Volume related to blood loss and effects from anesthesia.
Impaired Urinary Elimination related to birth trauma.
Constipation related to physiologic changes from birth.
Risk for Infection related to birth process.
Fatigue related to labor.
Acute Pain related to perineal discomfort from birth trauma, hemorrhoids, and physiologic changes from birth.
Readiness for Enhanced Self-health Management pertaining to postpartum care.
Readiness for enhanced parenting related to neonatal care.
Ineffective Breast-feeding related to lack of knowledge and inexperience.
Nursing Interventions
Monitoring for Hypotension and Bleeding
Monitor vital signs every 4 hours during the first 24 hours, then every 8 to 12 hours or as delineated by facility policy. Observe for the following:
Decreased respiratory rate below 14 to 16 breaths/minute may occur after receiving epidural opioids or opioid analgesics.
Increased respiratory rate greater than 24 breaths/minute may be caused by increased blood loss, pulmonary edema, or a pulmonary embolus.
Increased pulse rate greater than 100 beats/minute (bpm) may be present with increased blood loss, fever, or pain.
Decrease in blood pressure (BP) 15 to 20 mm Hg below baseline pressures may indicate decreased fluid volume or increased blood loss.
Assess the woman for light-headedness and dizziness when sitting upright or before walking.
Evaluate orthostatic BP.
Have the woman lie in bed if symptoms exist.
Emphasize the importance of asking for assistance before ambulating the first time.
Assess vaginal discharge for clots and amount.
Evaluate lower-extremity sensory function and motor function before ambulation if the woman had regional anesthesia.
Encourage food and drink, as tolerated.
Maintain IV line, as indicated.
Monitor postpartum hemoglobin levels and hematocrit.
Promoting Urinary Elimination
Observe for the woman’s first void within 6 to 8 hours after delivery.
Palpate the abdomen for bladder distention if the woman cannot void or if she complains of fullness after voiding.
Uterine displacement from the midline suggests bladder distention.
Frequent voidings of small amounts of urine suggest urine retention with overflow.
Catheterize the woman (in and out), if indicated.
Instruct the woman to void every several hours and after meals to keep her bladder empty. An undistended bladder may help decrease uterine cramping.
Promoting Proper Bowel Function
Teach the woman that bowel activity is sluggish because of decreased abdominal muscle tone, anesthetic effects, effects of progesterone, decreased solid food intake during labor, and prelabor diarrhea.
Inform the woman that pain from hemorrhoids, lacerations, and episiotomies may cause her to delay her first bowel movement.
Review the woman’s dietary intake with her.
Encourage adequate amounts of fresh fruit, vegetables, fiber, and at least eight glasses of water daily.
Encourage frequent ambulation.
Administer stool softeners, as indicated.
Preventing Infection
Observe for elevated temperature above 100.4° F (38° C).
Evaluate episiotomy/perineum for REEDA.
Assess for pain, burning, and frequency on urination.
Administer antibiotics as ordered.
Reducing Fatigue
Provide a quiet and minimally disturbed environment.
Organize nursing care to keep interruptions to a minimum.
Encourage the woman to minimize visitors and phone calls.
Encourage the woman to sleep while the baby is sleeping and specifically to nap or lie down and get off her feet at least 30 minutes per day.
Minimizing Pain
Instruct the woman to apply ice packs to her perineal area for the first 24 hours for perineal trauma or edema, then to apply heat to the area.
Take breaks between applications to prevent tissue damage.
Commercial or handmade packs of ice chips in a glove may be used.
Place a thin barrier between the ice pack and her skin.
Initiate the use of sitz baths for perineal discomfort after the first 24 hours.
Use three times per day for 15 to 20 minutes.
Instruct the woman to contract her buttocks before sitting to reduce perineal discomfort.
Assist the woman in the use of positioning cushions and pillows while sitting or lying.
Teach the woman to use a perineal bottle and squirt warm water against her perineum while voiding.
Provide pads with witch hazel or topical creams or ointments, as indicated.
Administer pain medication, as indicated.
Check breasts for signs of engorgement (swollen, tender, tense, shiny breast tissue).
If breasts are engorged and the woman is breastfeeding:
Allow warm-to-hot shower water to flow over the breasts to improve comfort.
Hot compresses on the breasts may improve comfort.
The application of cool cabbage leaves to the breast, left in place for 20 minutes, may reduce symptoms of engorgement.
Express some milk manually or by breast pump to improve comfort and to make the nipple more available for infant feeding.
Nurse the infant.
A mild analgesic may be used to enhance comfort.
If breasts are engorged and the mother is bottle-feeding:
Teach the woman to wear a snug, supportive bra night and day.
Teach the woman to avoid handling her breasts because this action stimulates more milk production.
Teach the woman to avoid letting warm water fall on her breasts during showers because the heat stimulates milk production.
Suggest the application of ice bags to the breasts to provide comfort.
Moderately strong analgesics may be needed to provide comfort.
Promoting Postpartum Health Maintenance
Teach the woman to perform perineal care—warm water over the perineum after each voiding and after each bowel movement several times per day to promote comfort, cleanliness, and healing.
Promote sitz baths for the same purpose.
Teach the woman to apply perineal pads by touching the outside only, thus keeping clean the portion that will touch her perineum.
Assess the condition of the woman’s breasts and nipples. Inspect nipples for reddening, erosions, or fissures. Reddened areas may be improved with vitamin A & D ointment, a lanolin cream (always remove before breastfeeding), and air-drying for 15 minutes, several times per day. She may also be instructed to squeeze a small amount of breast milk onto her nipples for lubrication.
Teach the woman to wash her breasts with warm water without soap, which prevents the removal of the protective skin oils.
Teach the woman to wear a bra that provides good support night and day.
Instruct the breastfeeding woman to add between 500 and 750 additional calories daily for milk production. Inform her that she also needs 2 to 3 quarts (2 to 3 L) of liquid per day; 20 g more protein than before pregnancy; additional calcium, phosphorus, and vitamins D, A, C, E, B, and B2; and additional niacin, zinc, and iodine.
Instruct the woman in postpartum exercises for the immediate and later postpartum period.
Immediate postpartum exercises can be performed in bed.
Toe stretch (tightens calf muscles)—while lying on your back, keep your legs straight and point your toes away from you, then pull your legs toward you and point your toes toward your chest. Repeat 10 times.
Pelvic floor exercise (tightens perineal muscles)—contract your buttocks for a count of 5 and relax. Contract your buttocks and press thighs together for a count of 7 and relax. Contract buttocks, press thighs together, and draw in anus for a count of 10 and relax.
Kegel exercises (tightens vaginal muscles)—contract vaginal muscles as if stopping stream of urine. Do 15 per day, increasing 5 more each week to a maximum of 40 per day. When conditioned, patient can do 4 or 5 Kegels per day for maintenance.
Abdominal breathing—lie on back, knees bent, hands on belly, feet flat. Suck in your belly, trying to pull your navel toward your spine. Hold 5 seconds; release. When you can do 10 (this can take a week), add a head lift. Suck in your belly, then hold it as you lift head toward chest, counting slowly to 4. Lower head for 4 slow counts; release belly. Muscles are working if fingers move down when you suck in belly, not up. Work up to 10 repetitions.
Arm circles—stand with feet approximately 12 inches (30.5 cm) apart, arms at sides. Keeping arms at sides, draw large circles with your shoulders by moving them forward, up, and back, and finish with a press down. Do 10 to 20 repetitions. Next, extend both arms as you reach forward, up, back, and down. Move slowly, breathe deeply for 5 to 10 repetitions.
Short walks—start with 5 minutes at first, then increase 5 minutes per day as desired.
Shoulder-side roll—lying on back, fold left arm across chest. Lift right arm and cross it over to left side. Feel as if your right arm is pulling you over so your right shoulder lifts and you roll to left. Continue to spiral movement as rib cage turns, then hips. Use left arm to take pressure off breasts, which may feel full. Lying on your left side, roll hips back toward right, followed by ribs, then shoulders until you are on your back. Repeat, other side. Perform five slow repetitions each side.
Exercises for the later postpartum period can be done after the first postpartum visit (1 to 2 weeks postpartum).
Bicycle (tightens thighs, stomach, and waist)—lie on your back on the floor, arms at sides, palms down. Begin rotating your legs as if you were riding a bicycle, bringing the knees all the way in toward the chest and stretching the legs out as long and as straight as possible. Breathe deeply and evenly. Do the exercises at a moderate speed and do not tire yourself.
Buttocks exercise (tightens buttocks)—lie on your stomach and keep your legs straight. Raise your left leg in the air, then repeat with your right leg (feel the contraction in your buttocks). Keep your hips on the floor. Repeat 10 times.
Twist (tightens waist)—stand with legs wide apart. Hold your arms at your sides, shoulder level, palms down. Twist your body from side to front and back again. Feel the twist in your waist.
Back bridge—begin by doing a pelvic tilt while lying on your back and flattening the lower back against the floor. Then continue to push your hips forward, lifting them off the floor. Hold the pelvic tilt for 4 seconds so that your back is flat, supporting your weight with your upper back. Lower your body slowly for 4 seconds so that upper back touches floor first, then waist touches, then pelvis.
All fours—begin on your hands and knees. First do a pelvic tilt, tucking in your buttocks and sucking in your belly. Do not allow your back to arch. Next, keeping your pelvic tilt, lift your left leg out behind you and extend your right arm in front of you. Slowly lower arm and leg. At first, you will have to work hard to keep your balance.
Lift and laugh—this is a fun exercise to do with your baby. Sit with legs crossed, back straight, belly sucked in. Cradle your baby in your folded arms and lift until your elbows are at shoulder height. Laugh and cuddle as you hold for 2 seconds. Slowly lower your baby, keeping shoulders even, if possible. Do 5 to 10 repetitions.
NURSING ALERT
Advise the mother to listen to her body. Avoid pain and fatigue. If pain or fatigue occurs, instruct the mother to stop her exercises. She may consult her obstetric provider, if desired.
Promoting Health Maintenance of the Neonate
Evidence Base
Cheffer, N. D., & Rannalli, D. A. (2011). Transitional care of the newborn. In S. Mattson & J. E. Smith (Eds.), Core curriculum for maternal-newborn nursing (4th ed., pp. 345-361). St. Louis, MO: Saunders Elsevier.
Encourage the parents to participate in the daily care of the infant.
Advise the parents to attend parenting and baby care classes offered during their stay at the birth facility.
Teach the parents to bathe and diaper the infant, perform circumcision care, and initiate either breast- or bottle-feeding.
Foster bonding by encouraging skin-to-skin contact with the infant (“kangaroo care”), eye contact, and talking to and touching the infant.
Instruct the parents to contact the infant’s health care provider for the following:
Fever above 100° F (37.8° C).
Loss of appetite for two consecutive feedings.
Inability to awaken the baby to his or her usual activity state.
Vomiting all or part of two feedings.
Diarrhea—three watery stools.
Extreme irritability or inconsolable crying.
Inform the parents that by law, infants and young children in cars are required to be in a car safety seat that is located in the back seat and that faces the back of the seat. Demonstrate and review the proper technique for use of the car seat.
Provide positive reinforcement and reassurance to the parents.
Provide written instructions and educational material on discharge.
Promoting Breastfeeding
Evidence Base
Orr, S. S. (2011). Breastfeeding. In S. Mattson & J. E. Smith (Eds.), Core curriculum for maternal-newborn nursing (4th ed., pp. 315-334). St. Louis, MO: Saunders Elsevier.
Assist the woman and infant in the breastfeeding process.
Have the mother wash her hands before feeding to help prevent infection.
Encourage the mother to assume a comfortable position, such as sitting upright in the bed or in a chair or lying on her side.
Have the woman hold the baby so that she is facing the mother. Common positions for holding the baby are the cradle hold, with the baby’s head and body supported against the mother’s arm, with buttocks resting in her hand; the football hold, in which the baby’s legs are supported under the mother’s arm, and the head is at the breast, resting in the mother’s hand; and lying on the side with the baby lying on his or her side facing the mother.
Teach the woman to bring the baby close to her to prevent back, shoulder, and arm strain.
Have the woman cup the breast in her hand in a C position, with bottom of the breast in the palm of her hand and the thumb on top; or the U position, with the fingers and the thumb to the sides of the breast and the breast resting in the palm of the hand.
Have the woman place her nipple against the side of the baby’s mouth, and when the mouth opens, guide the nipple and the areola into the mouth. The baby should latch on so that as much of the areola as possible is in his or her mouth. If the baby has latched on to the nipple only, take the baby off the breast by putting the tip of the mother’s finger in the corner of the baby’s mouth to break the suction, and then reposition on the breast to prevent nipple pain and trauma.
Encourage the woman to alternate the breast with which she begins feeding at each feeding to ensure emptying of both breasts and stimulation for maintaining milk supply.
Advise the mother to use each breast at each feeding. Begin with approximately 10 minutes at each breast, then increase the time at each breast, allowing the infant to suck until he or she stops sucking actively. Pinning a safety pin to the bra as a reminder of which breast to start with at the next feeding is helpful.
Have the mother breast-feed frequently (8 to 12 times/24 hours) to help maintain the milk supply. Although there is no time limit on each breastfeeding session, it is recommended to last at least 10 to 15 minutes on each breast.
Have the mother air-dry her nipples for approximately 15 to 20 minutes after feeding to help prevent nipple trauma.
Have the mother burp the infant at the end of the feeding to help release the air in the stomach and to make the infant less fretful.
Alert the mother that uterine cramping may occur, especially in multiparous women, because of the release of oxytocin, which can be worse in women with lessened uterine tone. Commonly referred to as afterpains.
Teach the mother to provide for adequate rest and to avoid tension, fatigue, and a stressful environment, which can inhibit the letdown reflex and make breast milk less available at feeding.
Advise the woman to avoid taking medications and drugs without health care provider approval because many substances pass into the breast milk and may affect milk production or the infant.
Evaluation: Expected Outcomes
Vital signs within normal limits; decreasing color and amount of lochia.
Voids freely and without discomfort.
Lack of constipation; eats high-fiber foods and uses stool softeners.
Afebrile, no abnormal redness of perineum, no purulent discharge or foul odor of lochia.
Verbalizes feeling rested.
Verbalizes decreased pain.
Incorporates postpartum care into activities of daily living.
Demonstrates confidence in performing infant care; shows signs of maternal-child bonding.
Demonstrates successful breastfeeding; breasts and nipples intact and without redness or cracks.
Postpartum Patient Education
Advise the woman that healing occurs within 2 to 4 weeks; however, evaluation by the health care provider during the follow-up visit is necessary.
Inform the woman that intercourse may be resumed when perineal and uterine wounds have healed and when vaginal bleeding has stopped. Inform the woman that normal vaginal secretions may not occur for up to 6 months. Also inform the mother that for the first 3 months following delivery, her sexual arousal and desire may be diminished due to infant needs and fatigue. Review methods of contraception. Sexual arousal may cause milk to leak from her breasts. Breastfeeding is not a reliable method of contraception.
Inform the woman that menstruation usually returns within 4 to 8 weeks if bottle-feeding; if breastfeeding, menstruation usually returns within 4 months, but may return between 2 and 18 months postpartum. Nursing mothers may ovulate even if they are experiencing amenorrhea. Thus, a form of contraception should be used if pregnancy is to be avoided.
Counsel the woman to rest for at least 30 minutes after she arrives home from the birthing facility and to rest several times during the day for the first few weeks.
Advise the woman to confine her activities to one floor if possible and to avoid stair climbing as much as possible for the first several days at home.
Counsel the woman to provide quiet times for herself at home and to help her establish realistic goals for resuming her own interests and activities.
Encourage the couple to provide times to reestablish their own relationship and to renew their social interests and relationships.
NURSING CARE OF THE NEONATE
Physiology of the Neonate
Evidence Base
Cheffer, N. D., & Rannalli, D. A. (2011). Transitional care of the newborn. In S. Mattson & J. E. Smith (Eds.), Core curriculum for maternal-newborn nursing (4th ed., pp. 345361). St. Louis, MO: Saunders Elsevier.
Verklan, M. T., & Walden, M. (Eds.). (2010). Core curriculum for neonatal intensive care nursing (4th ed.). St. Louis, MO: Saunders Elsevier.
The first 24 hours of life constitute a highly vulnerable time, during which the infant must make major physiologic adjustments to extrauterine life. Most neonates transition without difficulty during the first 6 to 10 hours of life.
Transitional Stages
During the period of postnatal transition, six overlapping stages have been identified:
Stage 1. Receives stimulation (during labor) from the pressure of the uterine contractions and from changes in pressure when the membranes rupture.
Stage 2. Encounters various foreign stimuli—light, cold, gravity, and sound.
Stage 3. Initiates breathing.
Stage 4. Changes from fetal circulation to neonatal circulation.
Stage 5. Undergoes alteration in metabolic processes, with activation of liver and GI tract for passage of meconium.
Stage 6. Achieves a steady level of equilibrium in metabolic processes (production of enzymes, increased blood oxygen saturation, decrease in acidosis associated with birth, and recovery of the neurologic tissues from the trauma of labor and delivery).
Respiratory Changes
Factors Initiating Respiration
Mechanical—pressure changes (eg, compression of the fetal chest with delivery) from intrauterine life to extrauterine life produce stimulation to initiate respirations.
Chemical—changes in the blood, as a result of transitory asphyxia, include:
Cessation of placental blood flow.
Lowered oxygen level.
Increased carbon dioxide level.
Lowered pH—if asphyxia is prolonged, depression of the respiratory center (rather than stimulation) occurs and resuscitation is necessary.
Sensory—light (visual), sound (auditory), olfactory, and tactile stimulation, beginning in utero with uterine contraction and when the infant is touched and dried, contribute to the initiation of respiration by stimulating the neonate’s respiratory center in the brain.
Thermal—a drop in environmental temperature from 98.6° F (37° C) to 70° to 75° F (21° to 23.9° C) produced by sudden chilling of the moist infant stimulates the respiratory center in the brain.
First breath—maximum effort is required to expand the lungs and to fill the collapsed alveoli.
Surface tension in the respiratory tract and resistance in lung tissue, thorax, diaphragm, and respiratory muscles must be overcome.
First active inspiration comes from a strong contraction of the diaphragm, which creates a high negative intrathoracic pressure, causing a marked retraction of the ribs and distention of the alveolar space. (Any remaining fluid is reabsorbed rapidly if the pulmonary capillary blood flow is adequate because the fluid is hypotonic and passes easily into the capillaries.)
Contributing factors, such as pulmonary blood flow, surfactant production, and respiratory musculature, also increase the respiratory effort of the neonate.
Character of Normal Respirations
First period of reactivity occurs immediately after birth. Vigorous, diffuse, purposeless movements alternate with periods of relative immobility/inactivity.
Respirations are rapid, as frequent as 80 breaths/minute, accompanied by tachycardia, 140 to 180 breaths/minute.
Relaxation occurs and the infant usually sleeps; he or she then awakes to a second period of activity. Oral mucus may be a major problem during this period.
Respirations are reduced to 30 to 60 breaths/minute and become quiet and shallow; respiration is carried out by the diaphragm and abdominal muscles.
Period of dyspnea and cyanosis may occur suddenly in an infant who is breathing normally; this may indicate an anomaly or a pathologic condition.
Pauses in respirations of less than 20 seconds are normal in the neonatal period.
Circulatory Changes
Cord clamping causes increased systemic vascular resistance (SVR), an increase in blood pressure, and increased pressures in the left side of the heart.
Removal of the placenta = functional closure of the ductus venosus shunt and anatomic closure the first week of life (see page 1258).
With the neonate’s first breath, the foramen ovale shunt closes. Permanent closure occurs by 3 months of age.
Increased SVR, falling pulmonary VR, and increased sensitivity to rising arterial oxygen concentrations in the blood = closure of ductus arteriosus shunt. The shunt is completely closed in all infants by 96 hours of age with permanent closure within 3 weeks to 3 months of age.
Blood volume can be as high as 300 mL/kg immediately after birth, then decrease to 80 to 85 mL/kg shortly after birth. Factors that influence blood volume:
Maternal blood volume (affected by maternal diseases and iron intake).
Placental function.
Uterine contractions during labor.
Amount of blood loss associated with delivery.
Placental transfusion at birth—increase in blood volume of 60% if cord is clamped and cut after pulsation ceases.
Residual cyanosis in hands and feet (acrocyanosis) is present for 1 to 2 hours after birth because of sluggish circulation.
Normal apical pulse rate 110 to 160 bpm; may rise to 180 bpm when the infant is crying or drop to 80 to 110 bpm during deep sleep.
BP is 65 to 95/30 to 60 mm Hg at birth (slightly higher in legs).
BP measurement is best accomplished with a Doppler device while the infant is at rest.
Coagulability is temporarily diminished because of lack of bacteria in the intestinal tract that contributes to the synthesis of vitamin K.
Coagulation time is 5 to 8 minutes (glass tubes), 5 to 15 minutes (room temperature), or 30 minutes (silicone tube).
Bleeding time is 2 to 4 minutes.
Prothrombin 50%, decreasing to 20% to 30% (approximately 13 to 18 seconds).
Values for blood components in the neonate:
Hemoglobin, 14.5 to 22 g/dL.
Hematocrit, 14% to 72%.
Reticulocytes, 4% to 6%.
Leukocytes, 9,000 to 34,000/mm3.
NURSING ALERT
A systolic BP in the upper extremities that is 20 mm Hg greater than in the lower extremities strongly suggests coarctation of the aorta.
Temperature Regulation
Mechanism not fully developed; heat production low.
Infant responds readily to environmental heat and cold stimuli.
Heat loss of 35.6° F to 37.4° F (2° C to 3° C) may occur at birth by radiation, convection, and evaporation.
Radiation—transfer of heat from neonate to cooler object not in direct contact with the infant.
Convection—transfer of heat when flow of cool air passes over infant’s skin.
Evaporation—loss of heat when water on infant’s skin is converted to vapor.
Conduction—transfer of heat when neonate comes into direct contact with cooler surface/object.
Decreased adipose tissue, thinner skin, blood vessels closer to the skin results in increased heat loss.
Infant develops mechanisms to counterbalance heat loss.
Vasoconstriction—blood directed away from skin surfaces.
Insulation—from subcutaneous adipose tissue.
Heat production—by nonshivering thermogenesis (brown fat metabolism) elicited by the sympathetic nervous system’s response to decreased temperatures; activated by adrenaline.
Fetal position—by assuming a flexed position.
Basal Metabolism
Surface area of infant, especially the head, is large in comparison to weight.
Basal metabolism per kilogram of body weight is higher than that of an adult.
Calorie requirements are high—117 calories per kilogram of body weight per day.
Renal Function
Neonatal kidneys have functional deficiency in concentrating urine and coping with fluid and electrolyte fluctuations. Low arterial BP and increased renal vascular resistance lead to the following effects:
Decreased ability to concentrate urine because of low tubular resorption rate and low levels of antidiuretic hormone.
Limited ability to maintain water balance by excretion of excess water or retention of needed water.
Decreased ability to maintain acid-base mechanism; slower excretion of electrolytes, especially sodium and hydrogen ions, results in accumulation of these substances, which predisposes the infant to dehydration, acidosis, and hyperkalemia.
Excretion of large amount of uric acid during neonatal period—appears as brick dust stain on diaper.
Hepatic Function
Only gold members can continue reading. Log In or Register to continue
 Evidence Base
Evidence Base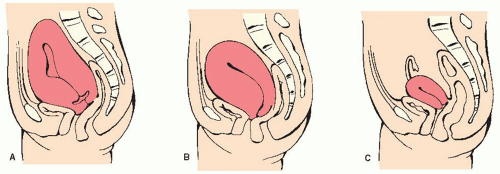
 NURSING ALERT
NURSING ALERT NURSING ALERT
NURSING ALERT NURSING ALERT
NURSING ALERT Evidence Base
Evidence Base Evidence Base
Evidence Base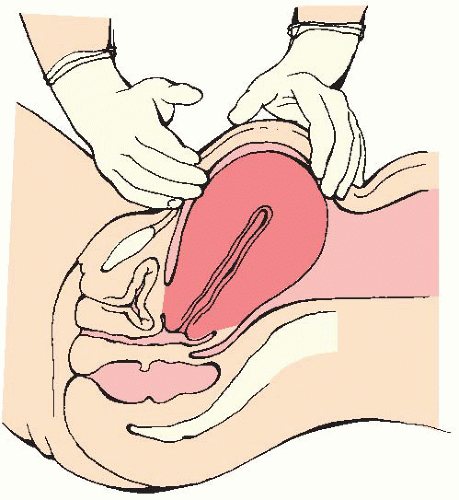
 Evidence Base
Evidence Base NURSING ALERT
NURSING ALERT Evidence Base
Evidence Base Evidence Base
Evidence Base Evidence Base
Evidence Base NURSING ALERT
NURSING ALERT


