Cancers of the Gastrointestinal Tract
Esophageal tumors are almost always malignant, accounting for 6% of all gastrointestinal cancers and 1% of all new cancers, and their incidence is rising at an alarming rate. It is more common in persons over 60 years of age, and it is the seventh leading cause of death among men.
Gastric cancer, one of the most common cancers worldwide, is more prevalent in developing countries among lower socioeconomic groups in urban settings. Japan, China, South America, and Eastern Europe have a high incidence, whereas the United States and Canada have a low incidence, approximately 1-2% of all new cancer cases annually. Immigrants acquire the same risk as natives, pointing to environmental factors in its development. Cancers in the antrum and body have been declining, whereas those of the cardia and gastroesophageal junction are increasing at an alarming rate. Causes are thought to be chronic Helicobacter pylori infection, genetic predisposition, and diet, especially diets with foods high in nitrates (bacon or hot dogs) and smoked, salted, or pickled foods. Other considered causes for gastric cancer include smoking and alcohol abuse.
Adenocarcinoma, also called colorectal cancer, is the second leading cause of cancer death in the United States and the most common type of cancer of the large bowel. Since the promotion of early detection, 5-year survival rates have risen to 60% but are much lower for low income groups, especially African-American males.
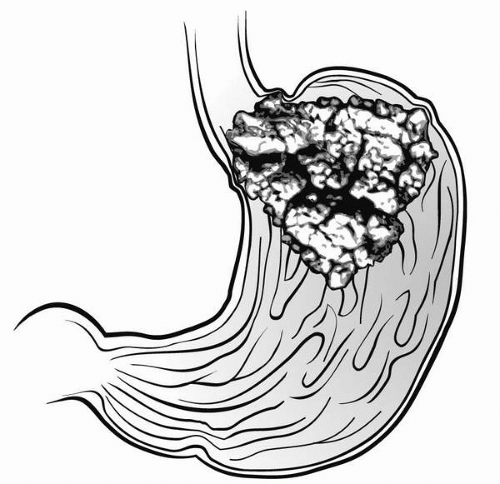 Figure 52-1 Carcinoma of the stomach. |
Carcinoma of the stomach arising from the gastric mucosa (see arrow) and extending into the esophagus. Risk factors include the following:
Dietary
Smoked foods
Pickled foods
Nitrates (contained in preservatives of prepared meats and in some drinking water supplies)
High salt intake
Nondietary
Altered anatomy after subtotal gastrectomy
Pathophysiology
Two types of cancer predominate. Squamous cell carcinoma, associated with the use of tobacco and alcohol, is more common in African-American males. Patients usually seek help because of progressive dysphagia for solids and then liquids, by which time the tumor is already inoperable.
Adenocarcinoma arises from columnar epithelium tissue and is associated with Barrett’s esophagus, which is a complication of chronic gastric esophagitis. This is found more commonly in whites in the distal one-third of the esophagus. Patients seek help for persistent gastroesophageal reflux that progresses to dysphagia. The tumor gradually narrows the lumen of the esophagus, infiltrates the surrounding tissues, and can invade the trachea, causing a tracheoesophageal fistula (Figure 52-1). Risk factors for esophageal cancer include cigarette smoking, alcohol abuse, gastroesophageal reflux, and poor diet.
Adenocarcinoma arises from columnar epithelium tissue and is associated with Barrett’s esophagus, which is a complication of chronic gastric esophagitis. This is found more commonly in whites in the distal one-third of the esophagus. Patients seek help for persistent gastroesophageal reflux that progresses to dysphagia. The tumor gradually narrows the lumen of the esophagus, infiltrates the surrounding tissues, and can invade the trachea, causing a tracheoesophageal fistula (Figure 52-1). Risk factors for esophageal cancer include cigarette smoking, alcohol abuse, gastroesophageal reflux, and poor diet.
 Adenocarcinoma arises from columnar epithelium tissue and is associated with Barrett’s esophagus, which is a complication of chronic gastric esophagitis.
Adenocarcinoma arises from columnar epithelium tissue and is associated with Barrett’s esophagus, which is a complication of chronic gastric esophagitis.Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Get Clinical Tree app for offline access
