Acute Respiratory Distress Syndrome and Pulmonary Emboli
This section provides an explanation of the pathophysiology related to acute respiratory distress syndrome and pulmonary emboli. Both of these conditions are life threatening.
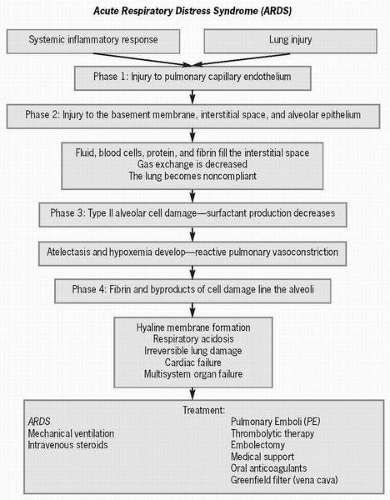 Figure 26-1 Acute respiratory distress syndrome. |
Acute respiratory distress syndrome (ARDS), also known as shock lung, wet lung, Vietnam lung, noncardiogenic pulmonary edema, and adult hyaline membrane disease, was first identified in 1967 as a cause of pulmonary edema resulting from alveolocapillary membrane injury. ARDS is an acute hypoxemia as the result of a systemic or pulmonary event that is not cardiac in origin. The patient with ARDS has widespread pulmonary infiltrates but a normal pulmonary capillary wedge pressure (below 18 mm Hg). This type of pulmonary edema affects approximately 150,000 patients per year and has a mortality rate of 30-40% and as high as 90% if the patient also is septic. Patients who survive ARDS may have permanent lung damage, and most have a persistent cough, dyspnea, and sputum production. Risk factors for developing this noncardiogenic pulmonary edema include aspiration of gastric contents, all types of shock, oxygen toxicity, fat embolism, major trauma, smoke inhalation, multiple blood transfusions, viral pneumonia, and burns. Approximately 3 in 10 patients who develop ARDS have had sepsis. Prevention of ARDS relies on avoidance of the occurrences that cause the syndrome.
 ARDS is an acute hypoxemia as the result of a systemic or pulmonary event that is not cardiac in origin.
ARDS is an acute hypoxemia as the result of a systemic or pulmonary event that is not cardiac in origin. This type of pulmonary edema has a mortality rate of 30-40% and as high as 90% if the patient also is septic.
This type of pulmonary edema has a mortality rate of 30-40% and as high as 90% if the patient also is septic.Any bolus of bloodborne material such as air from an intravenous line, fat from a long bone fracture or trauma, amniotic fluid that enters the circulation during childbirth, tumor tissue, or a thrombus that blocks a pulmonary artery is termed a pulmonary embolism (PE), the third most common cardiovascular disease process in the United States. Approximately 64% of autopsies reveal a PE regardless of the cause of death. PE causes a sudden obstruction of blood flow to lung tissue and may cause death, especially within the first 1 to 2 hours after the initial insult. The most common sources of blood clots include the right ventricle, as a consequence of atrial fibrillation, and deep vein thrombosis arising in the pelvis or calf muscles. Deep vein thrombosis is the most common cause of PE, accounting for approximately 5 million cases in the United States each year. Annually, PE is
responsible for approximately 200,000 deaths and is the third leading cause of death among hospitalized patients. Over half of patients with proximal deep vein thrombosis develop PE, many of which are asymptomatic.
responsible for approximately 200,000 deaths and is the third leading cause of death among hospitalized patients. Over half of patients with proximal deep vein thrombosis develop PE, many of which are asymptomatic.
 Approximately 64% of autopsies reveal a PE regardless of the cause of death.
Approximately 64% of autopsies reveal a PE regardless of the cause of death. Deep vein thrombosis is the most common cause of PE.
Deep vein thrombosis is the most common cause of PE. PE causes a sudden obstruction of blood flow to lung tissue and may cause death, especially within the first 1 to 2 hours after the initial insult.
PE causes a sudden obstruction of blood flow to lung tissue and may cause death, especially within the first 1 to 2 hours after the initial insult. Over half of patients with proximal deep vein thrombosis develop PE, many of which are asymptomatic.
Over half of patients with proximal deep vein thrombosis develop PE, many of which are asymptomatic.Prevention of PE lies in removing or reducing risk factors that create clots. Risk factors that create Virchow’s triad (venous stasis, vessel wall injury, hypercoagulability) such as bed rest, polycythemia, and pregnancy, may lead to a PE. Low-dose subcutaneous heparin every 12 hours helps to reduce the likelihood of deep vein thrombosis after surgery or during periods of immobility. Some of the measures used to reduce the risk of PE are encouraging movement and using sequential compression devices (Venodyne boots) in postoperative or bed-ridden patents, avoiding oral contraceptives in women who smoke, using anticoagulant medication for patients with atrial fibrillation, and using an inferior vena cava filter (Greenfield filter) to stop clots from traveling to the heart.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


